Mar 31, 2026

What if the spot you choose for your weekly injection is quietly undermining your results? It is a question that haunts thousands of semaglutide users. You pick a spot, press the needle in, and hope for the best. But does it actually matter where the needle goes?
The answer is more nuanced than most guides admit. The injection site you choose does influence how quickly semaglutide begins working, how comfortable the experience feels, and whether you develop long-term complications at the injection area. But here is the part that surprises most people: the differences between approved sites are small enough that the FDA considers them clinically equivalent. What matters far more than choosing the "perfect" spot is mastering technique, rotating consistently, and avoiding a handful of common mistakes that genuinely do reduce effectiveness.
This guide breaks down everything researchers and clinicians know about semaglutide injection sites, from the measurable absorption differences between your abdomen, thigh, and upper arm, to the rotation strategies that prevent tissue damage, to the technique details that separate a clean injection from a painful one. Whether you are on your first week of semaglutide or months into your protocol, the information here will help you get the most from every dose. SeekPeptides has compiled the research, the clinical guidelines, and the practical wisdom that experienced users have learned through thousands of injections.
The three approved injection sites for semaglutide
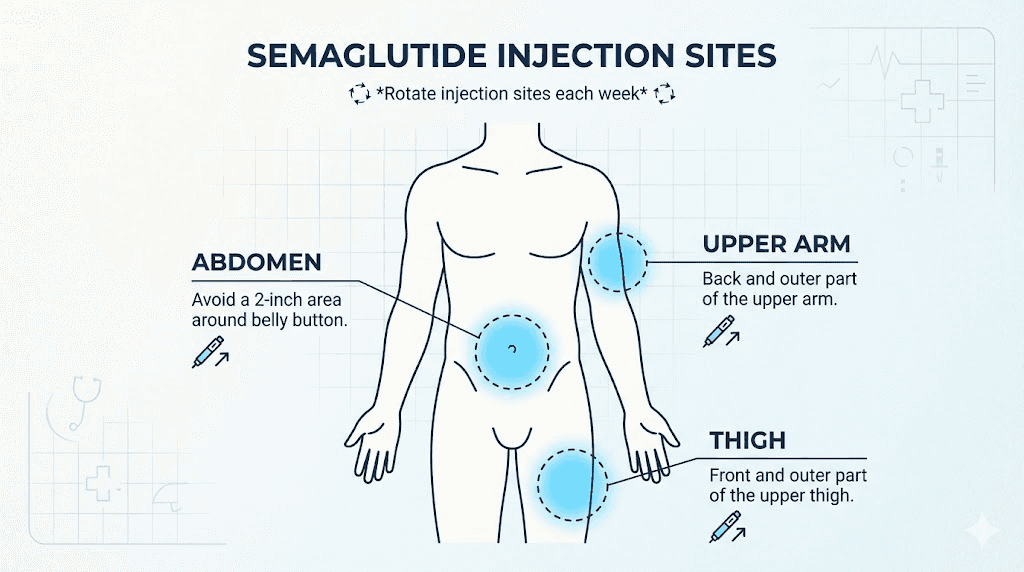
Semaglutide is a subcutaneous injection. That means it goes into the layer of fat just beneath the skin, not into muscle or vein. The FDA and Novo Nordisk approve three specific body areas for administration. Each one works. Each one delivers the medication into your system. But each one has characteristics worth understanding before you choose.
Knowing your options matters because different sites suit different body types, comfort preferences, and daily routines. Some people find one location consistently easier than others. Some discover that rotating between all three gives them the best long-term experience. The key is understanding what makes each site unique so you can make informed decisions rather than guessing.
The abdomen
The abdomen is the most popular injection site for semaglutide, and for good reason. This area typically has a generous layer of subcutaneous fat, which makes needle insertion straightforward and relatively painless. The correct semaglutide dose absorbs consistently from abdominal tissue because blood flow to this region is reliable and the fat layer is uniform in most people.
The injection zone covers a wide area. You can use anywhere on your abdomen that is at least two inches away from your navel. Avoid the area directly around the belly button because the tissue composition changes there, and absorption becomes less predictable. Also avoid any area with visible veins, moles, scars, or stretch marks.
Most clinicians recommend the abdomen as the starting point for new users. The large surface area gives you plenty of room for tracking and rotating your injection sites week to week. And the fat layer here tends to be thick enough that even users with lower body fat percentages can inject comfortably without hitting muscle.
The outer thigh
The front and outer portion of the thigh is the second approved site. This area works well for people who find abdominal injections uncomfortable or who want to give their stomach area a break during rotation cycles. The thigh injection technique follows similar principles to abdominal injection but requires slightly different positioning.
Use the middle third of the outer thigh. Too high and you risk injecting near the hip joint area where tissue composition changes. Too low and you approach the knee where subcutaneous fat thins dramatically. The sweet spot is roughly a hand width above the knee and a hand width below the hip, along the outer edge of the leg.
One important consideration: research suggests that bioavailability may be up to 12% lower when injecting into the thigh compared to the abdomen. We will explore what this means practically in a later section. For now, know that this difference exists but is not considered clinically significant by the FDA or by Novo Nordisk.
The upper arm
The back of the upper arm is the third approved location.
This site works best when someone else administers the injection because reaching your own upper arm at the correct angle can be awkward. If you are self-injecting, the abdomen or thigh are generally more practical choices.
The target area is the fatty part on the back of the arm, roughly halfway between the shoulder and elbow. Avoid the inner arm where veins are more prominent and the skin is thinner. This location has moderate subcutaneous fat in most people, though very lean individuals may find the fat layer insufficient here.
The upper arm absorption rate falls between the abdomen and thigh. Clinical observations show consistent delivery from this site, and many users who inject with a partner prefer it because the process is quick and the area is easily accessible to another person. For proper syringe injection technique, the upper arm requires the same 90-degree angle and full needle insertion as other sites.
How injection site affects absorption
Here is where the science gets interesting. Different body areas do absorb semaglutide at slightly different rates. This is not unique to semaglutide. It applies to virtually all subcutaneous medications. The reason comes down to blood flow, fat layer thickness, and tissue composition at each location.
But "different" does not mean "dramatically different." And that distinction matters enormously for anyone worried about choosing the wrong spot.
Bioavailability differences between sites
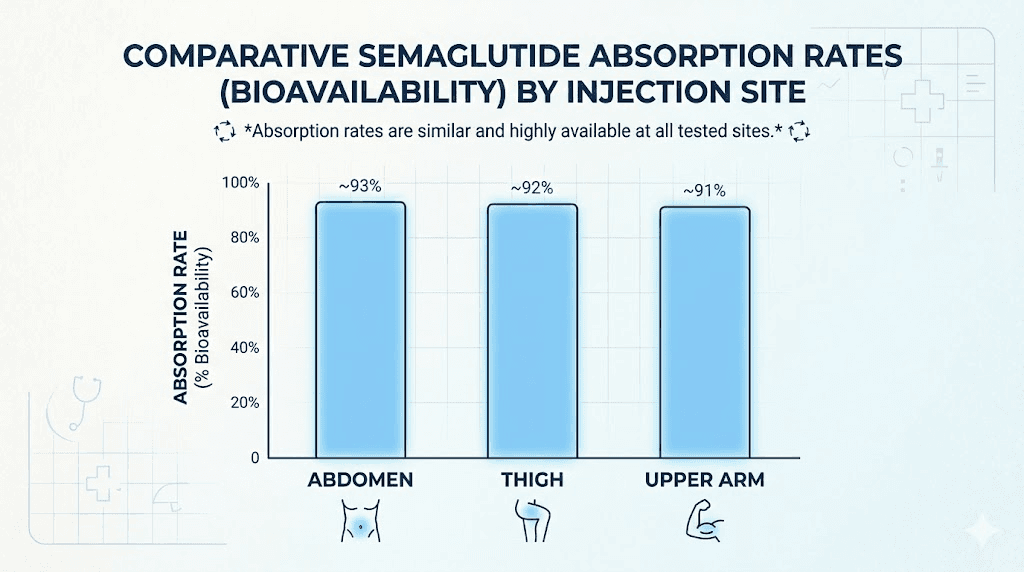
Bioavailability refers to the percentage of a medication that actually reaches your bloodstream and becomes active in your body. For subcutaneous semaglutide, the maximum bioavailability is approximately 89%, regardless of injection site. That means about 89% of the dose you inject makes it into systemic circulation.
The differences between sites are real but small. Research indicates that thigh injections may produce bioavailability up to 12% lower than abdominal injections. The upper arm falls somewhere in between. To put this in perspective, if you inject 0.5 mg into your abdomen and roughly 0.445 mg reaches your bloodstream, injecting the same dose into your thigh might deliver roughly 0.392 mg. That is a measurable gap, but the clinical impact is negligible for most users because semaglutide has a long half-life and accumulates in the body over weeks of consistent dosing.
Novo Nordisk prescribing information states that "similar exposure" is achieved across all three approved injection sites. The FDA reviewed these differences during the approval process and determined they do not require dose adjustments based on injection location. Your semaglutide dosage chart remains the same whether you inject in your stomach, thigh, or arm.
Why the abdomen absorbs faster
The abdomen leads in absorption speed for a straightforward physiological reason. This region has higher blood flow to the subcutaneous tissue compared to the thigh or upper arm. More blood flow means the medication gets picked up and distributed through the body more quickly.
The subcutaneous fat in the abdominal area also tends to be more vascularized, meaning it has a denser network of small blood vessels running through it. When semaglutide is deposited into this well-supplied tissue, it enters the bloodstream efficiently. The thigh, by contrast, has comparatively lower blood perfusion in the subcutaneous layer, which is why absorption from this site tends to be slightly slower.
Temperature plays a role too. The abdomen stays relatively warm because it is close to core body temperature. The thigh and upper arm, being extremities, can be cooler, and cooler tissue means slightly slower blood flow and absorption. This effect is minor but contributes to the overall difference between sites.
Does faster absorption mean better results
No. This is one of the most common misconceptions about injection sites.
Faster absorption does not equal better weight loss, stronger appetite suppression, or superior blood sugar control. Semaglutide is a once-weekly medication specifically because it has an extremely long half-life of approximately seven days. The medication builds up in your system over four to five weeks of consistent dosing until it reaches what pharmacologists call "steady state," a stable concentration that remains relatively constant between doses.
At steady state, whether the most recent dose absorbed in 4 hours or 8 hours makes virtually no difference to your overall blood levels. The reservoir of semaglutide already circulating in your body is so much larger than any single weekly dose that small absorption speed differences wash out completely. This is why the week-by-week results of semaglutide remain consistent regardless of which site you use, as long as you are injecting the correct dose at regular intervals.
Think of it like filling a swimming pool with a garden hose. Whether the water flows at 10 gallons per minute or 11 gallons per minute, the pool fills to the same level. The tiny difference in flow rate becomes irrelevant against the massive volume already in the pool.
Why site rotation matters more than site selection
If there is one takeaway from this entire guide, it is this: rotating your injection site is dramatically more important than choosing the "best" site. The research is clear. Proper rotation prevents complications that can genuinely undermine semaglutide effectiveness. Choosing the abdomen over the thigh gives you a marginal absorption advantage. Failing to rotate gives you real problems.
What happens when you do not rotate
When you inject into the same small patch of skin week after week, the tissue underneath begins to change. The body responds to repeated needle trauma by altering the local fat composition. Collagen deposits accumulate. Small areas of scar tissue form. The subcutaneous fat can thicken in spots or thin out in others. These changes happen gradually, often over months, and many users do not notice them until the damage is significant.
The Cleveland Clinic reports that as many as two-thirds of people who require regular injections develop lipohypertrophy at some point. That is not a rare complication. It is the expected outcome of poor rotation habits. And the consequences go beyond cosmetics.
Lipohypertrophy and absorption problems
Lipohypertrophy refers to lumpy, firm patches or balls of fatty tissue that form under the skin at overused injection sites. These growths look like small, rubbery bumps and can persist for weeks or months after you stop injecting in that area.
The real danger of lipohypertrophy is not the lumps themselves. It is what they do to medication absorption. Lipohypertrophic tissue has altered blood supply and different structural properties than healthy subcutaneous fat. When you inject semaglutide into one of these damaged areas, absorption becomes unpredictable. Sometimes the medication absorbs faster than expected. Sometimes slower. Sometimes it pools in the tissue and releases erratically over days.
This unpredictability can make your carefully calculated semaglutide dosage effectively unreliable. You might experience stronger side effects one week and reduced effectiveness the next, all because the tissue at your injection site is damaged. Users who report that their compounded semaglutide is not working or that they have hit a semaglutide plateau should consider whether injection site issues might be contributing to inconsistent results.
Lipoatrophy, the opposite condition where fat tissue breaks down and leaves indentations in the skin, can also occur with repeated injection in the same spot. Both conditions compromise the integrity of the subcutaneous layer and reduce reliable medication delivery.
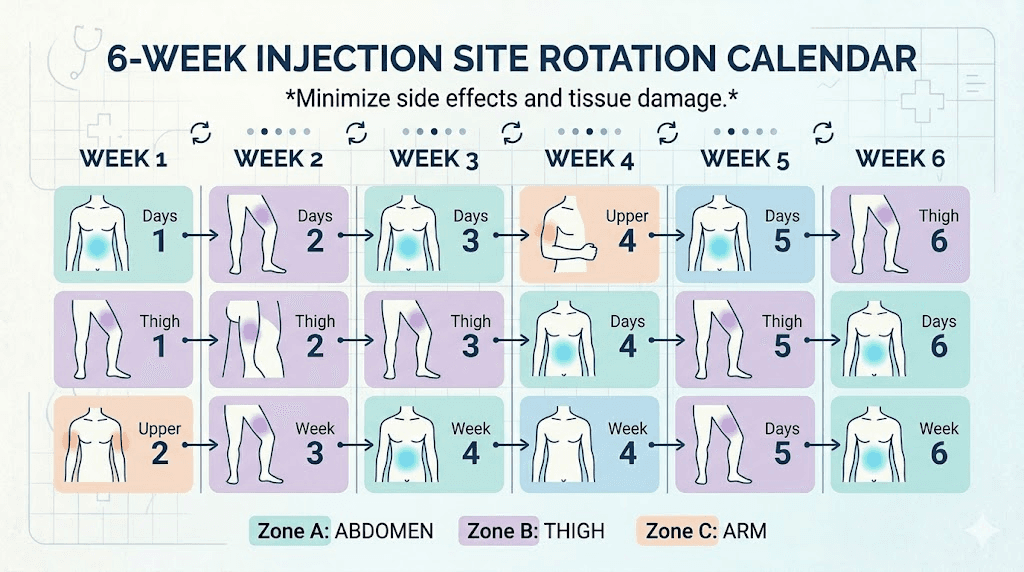
A practical rotation schedule
The simplest effective rotation strategy uses a three-zone cycle that moves between body areas every week.
Week 1: Abdomen, right side
Week 2: Left thigh, outer portion
Week 3: Abdomen, left side
Week 4: Right thigh, outer portion
Week 5: Abdomen, right side (several inches from the Week 1 spot)
Week 6: Left thigh, different spot from Week 2
If you have a partner who can help, add the upper arm into the rotation for even more variety. The goal is simple: never inject within one inch (2.5 cm) of your previous injection site, and ideally use a completely different body area each week.
Some users find it helpful to track their injection sites with a simple log or body diagram. Mark where you injected each week so you can see at a glance which areas need rest and which are available. After a few months, this becomes second nature, but in the beginning, a tracking system prevents accidentally overusing one spot.
Injection technique that actually matters
Beyond choosing a site and rotating properly, the way you physically perform the injection has a meaningful impact on comfort, absorption, and complication risk. Poor technique can turn an easy weekly routine into a dreaded experience. Good technique makes the process nearly painless and maximizes medication delivery.
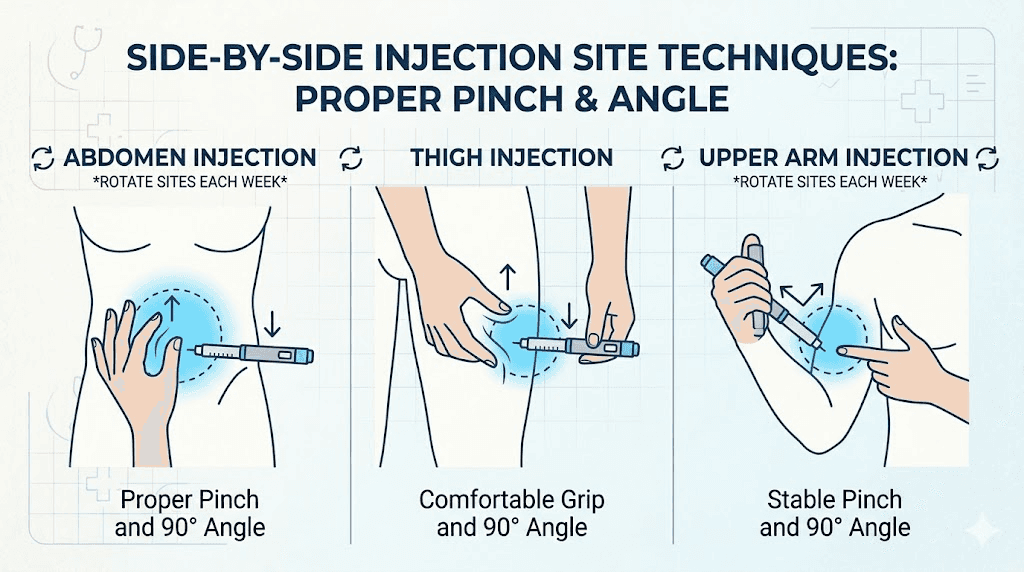
Proper depth and angle
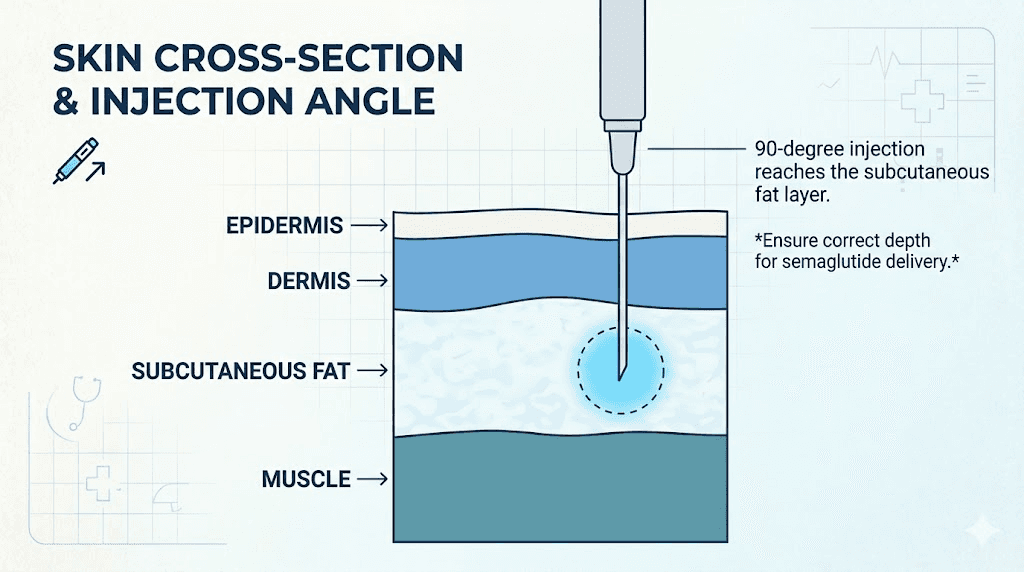
Semaglutide must reach the subcutaneous fat layer to absorb correctly. Inject too shallow and the medication stays in the dermis, causing irritation, redness, and poor absorption. Inject too deep and you hit muscle tissue, which changes the absorption rate and can cause more pain.
The standard technique is straightforward. Insert the needle at a 90-degree angle, perpendicular to the skin surface. If you are using an Ozempic pen, the 4mm needle is designed to penetrate through the epidermis and dermis directly into the subcutaneous layer for most body types. For people using insulin syringes with compounded semaglutide, needle length typically ranges from 4mm to 8mm, and the same 90-degree insertion applies.
If you accidentally inject semaglutide into muscle, do not panic. The medication will still absorb, but potentially at a different rate, and the injection site may be more sore than usual. It is not dangerous, but it is not ideal. Consistent subcutaneous delivery provides the most predictable pharmacokinetic profile.
The skin pinch method
People with lower body fat percentages may not have a thick enough subcutaneous layer for direct 90-degree insertion, especially on the thigh or upper arm. In these cases, the skin pinch technique helps.
Gently gather a fold of skin between your thumb and forefinger. This lifts the subcutaneous fat away from the underlying muscle and creates a thicker target for the needle. Insert the needle into the center of this fold at a 90-degree angle, or at a 45-degree angle if the fold is thin.
Hold the pinch throughout the injection and for a few seconds after removing the needle. This keeps the tissue elevated and ensures the medication deposits into the fat layer rather than dispersing into deeper tissue. The skin pinch is especially useful on the thigh, where the subcutaneous layer can be thinner than the abdomen in many people.
How long to hold the needle
After pressing the injection button on a semaglutide pen, hold the needle in place for at least 10 seconds before withdrawing. This is not optional. It is not a suggestion.
The 10-second hold allows the full dose to leave the pen cartridge and deposit into the tissue. Removing the needle too early can result in medication leaking out of the injection site, which means you receive less than the intended dose. Some users notice a small droplet of liquid at the injection site after removing the needle. A tiny amount is normal. A visible stream or large drop suggests the needle was removed too quickly.
For users injecting with a syringe rather than a pen, the same principle applies. After depressing the plunger completely, hold the needle in place for 5-10 seconds before withdrawing. This gives the medication time to spread into the surrounding tissue rather than tracking back up the needle channel.
Common injection site problems and how to fix them
Even with perfect technique and consistent rotation, injection site reactions happen. Most are mild and resolve on their own. Some require attention. Knowing the difference helps you respond appropriately and avoid unnecessary worry.
Injection site reactions occur in roughly 1.4% to 2.4% of patients using subcutaneous semaglutide, according to clinical trial data. That makes them uncommon but not rare. Understanding what is normal and what warrants a call to your healthcare provider keeps you confident in your protocol.
Redness and swelling
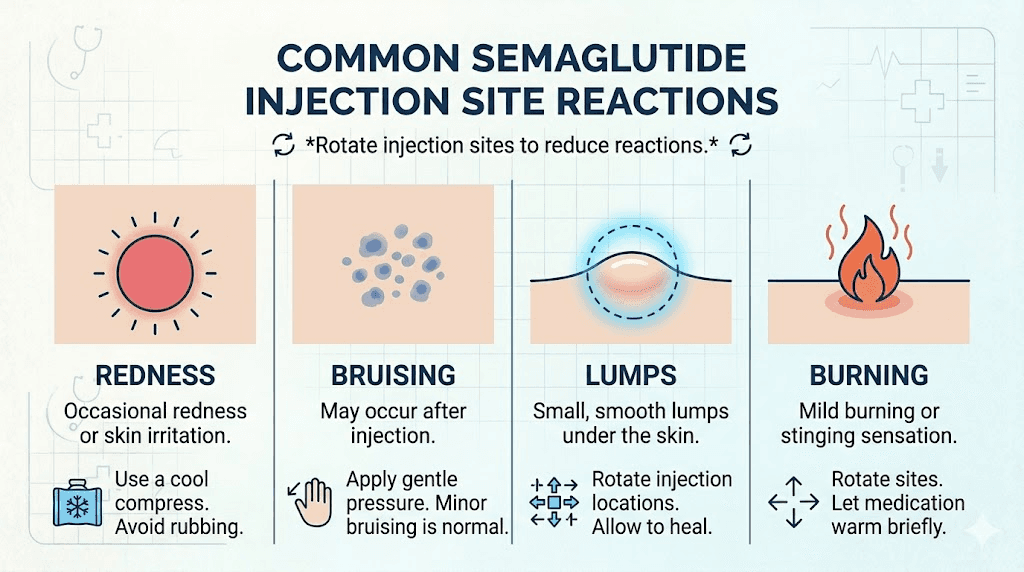
Mild redness around the injection site is the most common reaction. It typically appears within an hour of injection and resolves within 24 to 48 hours. The redness comes from the needle causing minor tissue trauma and a small localized inflammatory response. This is your body doing exactly what it should do.
To minimize redness, let the alcohol swab dry completely before injecting. Wet alcohol on the skin can be carried into the tissue by the needle, causing more irritation.
A cold compress applied for 5-10 minutes after injection can reduce both redness and any accompanying swelling. Over-the-counter antihistamines may help if the redness is accompanied by itching.
If redness persists beyond 48 hours, spreads significantly, or is accompanied by warmth and increasing tenderness, contact your healthcare provider. These could be signs of infection rather than a normal injection site reaction.
Bruising
Bruising happens when the needle nicks a small blood vessel beneath the skin. It looks alarming but is harmless. The bruise will change color over several days and disappear within one to two weeks.
To reduce bruising risk, avoid areas where you can see veins through the skin. Do not rub or massage the injection site immediately after injecting, as this can worsen bleeding from any nicked vessels. Apply gentle pressure with a cotton ball for 30-60 seconds after removing the needle.
Frequent bruising in the same general area may indicate that you are not rotating enough. Move to a completely different zone if one area seems prone to bruising. Users taking blood thinners or fish oil supplements may bruise more easily and should discuss injection strategies with their provider. The same considerations apply to semaglutide and liver function, where medication interactions can affect how your body responds to the injection.
Lumps under the skin
A study published in the Journal of Diabetes Investigation documented injection-site nodules associated with once-weekly subcutaneous semaglutide. These nodules present as small, firm lumps under the skin at the injection site. They usually resolve within days to weeks without treatment.
Nodules can form when the injected solution pools in the tissue rather than dispersing evenly. This is more common with larger volume injections or when the needle is removed too quickly. Ensuring proper injection depth and holding the needle for the recommended 10 seconds reduces the risk significantly.
If lumps persist for more than two weeks, increase in size, become painful, or show signs of infection (redness, warmth, pus), seek medical evaluation. Persistent lumps may also indicate early lipohypertrophy, which is a signal to stop injecting in that area and improve your rotation habits.
Burning or stinging
Some users report a burning or stinging sensation during or immediately after injection. This can have several causes. Cold medication straight from the refrigerator stings more than room-temperature medication. Allow your semaglutide to sit at room temperature for 15-30 minutes before injecting. The storage guidelines for semaglutide allow the medication to remain at room temperature (up to 86 degrees Fahrenheit) for limited periods, so brief warming is safe.
Rapid injection can also cause burning. Push the plunger or press the pen button at a steady, moderate speed rather than forcing the medication in quickly. Slower injection allows the tissue to accommodate the incoming fluid gradually, reducing pressure and discomfort.
A lingering burn that lasts more than a few minutes could indicate the needle reached a nerve-rich area or that the injection went too shallow into the dermal layer. Adjusting your injection site by even an inch can make a significant difference in comfort.
Mistakes that reduce semaglutide effectiveness
Some injection habits do not just cause discomfort. They actively reduce how well semaglutide works. These are the mistakes worth eliminating from your routine because they can explain why you are not losing weight on semaglutide even when you are doing everything else right.
Injecting into muscle instead of fat
Muscle tissue has dramatically different blood flow characteristics than subcutaneous fat. Intramuscular injection causes semaglutide to absorb much faster than intended, which can increase side effects like bloating, dizziness, and fatigue while potentially reducing the duration of the medication effect between doses.
The risk of hitting muscle is highest on the thigh and upper arm where the subcutaneous layer can be thin, especially in lean or athletic individuals. Using the skin pinch technique, choosing appropriate needle length, and inserting at the correct angle all help ensure proper subcutaneous placement.
If you consistently experience more intense side effects after thigh or arm injections compared to abdominal injections, depth issues may be the cause. Consider switching to abdominal injections where the fat layer is typically thicker, or speak with your provider about needle length options.
Using the same spot every week
This is the single most damaging injection habit. We covered lipohypertrophy in detail earlier, but it bears repeating. The same spot every week means the same patch of tissue absorbs medication, experiences needle trauma, and undergoes inflammatory response 52 times per year. No tissue in your body is designed for that.
Even moving just two inches from your last injection site makes a meaningful difference. But ideally, you should alternate between completely different body zones, giving each area at least two to three weeks of rest between injections. Discipline with rotation is one of those invisible habits that separates users who get consistent semaglutide results from those who plateau or develop complications.
Injecting into scarred or damaged tissue
Scar tissue, stretch marks, and areas of previous injury have altered blood supply and tissue structure. Medication absorption from these areas is unreliable. You might absorb 90% of the dose from healthy tissue and only 50% from scarred tissue, creating the kind of inconsistency that undermines predictable results.
Inspect your injection site before each use. The skin should be healthy, smooth (relatively), and free from visible damage. Avoid areas with surgical scars, burn marks, heavy stretch marks, or previously injured tissue. If a significant portion of your abdomen has stretch marks, focus on the areas that remain clear, or use your thigh and arm more frequently in your rotation.
Injecting through clothing
It sounds obvious, but it happens. Never inject through fabric. Clothing fibers can be pushed into the skin by the needle, introducing contaminants and increasing infection risk. The alcohol swab cleaning step also becomes impossible through clothing. Always expose the injection site completely before cleaning and injecting.
Skipping the alcohol swab
Cleaning the injection site with an alcohol swab before injecting is a basic infection prevention step. It removes surface bacteria that could be pushed into the subcutaneous tissue by the needle. Skipping this step occasionally might not cause problems, but making it a habit significantly increases your cumulative infection risk over months and years of weekly injections.
Site-specific tips for each injection location
Each of the three approved injection sites has its own practical considerations. These tips come from clinical guidelines and the collective experience of thousands of semaglutide users. Mastering the nuances of each location makes your rotation cycle smoother and more comfortable.
Abdomen injection guide
The abdomen offers the largest usable area and the most forgiving fat layer. Here is how to get the most from abdominal injections.
Preparation: Stand or sit with your abdominal muscles relaxed. Tensing the muscles pushes the subcutaneous fat layer closer to the underlying tissue and can make the injection more painful. Take a breath and let your stomach relax naturally.
Site selection: Imagine a large oval around your navel, starting two inches out from the belly button and extending to your sides. The entire area within this oval (except the two-inch exclusion zone around the navel) is fair game. You have dozens of potential injection points.
Technique: For most people, direct 90-degree insertion without a skin pinch works perfectly on the abdomen. The fat layer here is thick enough to accommodate standard needle lengths comfortably. If you are very lean, a gentle pinch may help.
Rotation within the abdomen: Divide the area into quadrants, upper right, upper left, lower right, lower left, and cycle through them. Each quadrant has enough space for multiple injection points that are at least one inch apart. This gives you roughly 12-16 unique spots on the abdomen alone before you need to revisit any area.
If you are following a semaglutide diet plan and losing significant abdominal fat, you may notice the subcutaneous layer thinning over time. Monitor your injection comfort and adjust technique (add a skin pinch) or shift to the thigh more frequently as your body composition changes.
Thigh injection guide
The thigh requires a bit more attention to positioning but provides an excellent secondary site for your rotation schedule.
Preparation: Sit on a chair or the edge of a bed with your thigh relaxed and your foot flat on the floor. This position naturally relaxes the quadriceps muscle and allows the subcutaneous fat to separate from the muscle beneath it. Avoid injecting while standing, as this tenses the thigh muscles and thins the fat layer.
Site selection: Target the middle third of the outer thigh. You can also use the front of the thigh if you have adequate fat there, but the outer aspect is preferred because the subcutaneous layer tends to be thicker. Avoid the inner thigh where major blood vessels run close to the surface.
Technique: Many users benefit from the skin pinch technique on the thigh, especially if they carry less fat in this area. Pinch a fold of skin and fat, insert the needle at 90 degrees into the center of the fold, and hold the pinch throughout the injection.
Special consideration: Athletic or lean individuals may find the thigh challenging due to minimal subcutaneous fat. If you can feel muscle immediately beneath the skin when you pinch, the thigh may not be your best option. In this case, focus your rotation on the abdomen and upper arm instead.
Upper arm injection guide
The upper arm is best suited for partner-assisted injection but can work for self-injection with practice.
Preparation: Let your arm hang naturally at your side. Do not flex. The target area is the back of the upper arm, roughly in the center between shoulder and elbow. If self-injecting, you may need to use a mirror or practice the motion to build confidence.
Site selection: Focus on the tricep area, the back and outer portion of the upper arm. Avoid the inner arm and areas near the elbow or shoulder joint. The fat layer here varies significantly between individuals. Pinch the area to assess whether you have enough subcutaneous tissue for a comfortable injection.
Technique: The skin pinch is recommended for most upper arm injections. Gather a fold of tissue with your free hand (or have your partner do this), insert the needle, inject, hold for 10 seconds, then remove. If self-injecting, some users find it easier to sit the arm on a table or rest it against their body for stability.
When to choose the arm: The upper arm is ideal for people who have developed sensitivity or tissue changes in the abdomen and thigh after months of use. Adding it to your rotation gives overused areas more recovery time. It is also the preferred site for many healthcare providers when administering injections in clinical settings.
How body composition affects injection site choice
Your body type matters. Not all injection sites work equally well for all people, and understanding how your individual anatomy affects the injection experience helps you make smarter choices.
Higher body fat percentages
People with higher body fat percentages generally have the easiest time with subcutaneous injections. The generous fat layer at all three approved sites means reliable absorption, comfortable needle insertion, and plenty of room for rotation. The abdomen is typically the most convenient site, but the thigh and upper arm also work well.
One consideration for larger-bodied individuals: ensure the needle is long enough to reach the subcutaneous layer. Very short needles (4mm) may not fully penetrate the dermis in areas with exceptionally thick skin. Your healthcare provider can recommend the appropriate needle length for your body type. The GLP-1 syringe guide covers needle selection in detail.
Lower body fat percentages
Lean individuals face the opposite challenge. The subcutaneous layer may be thin enough that standard injection technique risks intramuscular delivery, particularly on the thigh and upper arm. The abdomen is usually the safest site for lean users because it retains subcutaneous fat even at lower overall body fat percentages.
Always use the skin pinch technique if you are lean. Shorter needles (4mm) are preferable to longer ones. And if you notice consistently more pain, deeper bruising, or stronger side effects when injecting in the thigh or arm, switch to abdomen-only injections and discuss alternative sites with your provider.
As your body changes on semaglutide, your injection experience may change too. Many users begin with ample subcutaneous fat and find that after months of significant weight loss on semaglutide, previously comfortable sites become trickier. Adapt your technique as your body evolves. This is a dynamic process, not a set-it-and-forget-it decision.
Post-surgical or scarred areas
Surgical scars, C-section scars, liposuction areas, and significant burn scars all alter the subcutaneous tissue structure. Absorption from these areas is unpredictable. Mark them as no-go zones in your rotation plan and choose alternative spots with healthy tissue.
Tattoos, by contrast, do not generally affect absorption. The ink sits in the dermal layer, above the subcutaneous fat. Injecting through a tattooed area is acceptable, though some users prefer to avoid it for aesthetic reasons.
Temperature, timing, and other factors that matter
The injection site is just one variable in the equation. Several other factors influence your injection experience and semaglutide absorption.
Medication temperature
Cold semaglutide stings more than room-temperature semaglutide. If your medication comes from the refrigerator, let it warm up for 15-30 minutes before injecting. You can hold the pen or vial in your hands for a few minutes to speed the process. Do not use a microwave, hot water, or any heat source to warm the medication, as excessive heat degrades semaglutide and can reduce its effectiveness.
Understanding how long semaglutide lasts in the fridge and its shelf life helps you manage storage properly. Medication that has been compromised by temperature extremes may not deliver consistent results regardless of injection technique.
Time of day
Does it matter when you inject? The best time of day to take semaglutide is whatever time you can commit to consistently. The medication effect is not significantly different between morning and evening injections. However, some users find that injecting in the evening helps them sleep through the initial hours when side effects are most likely to appear.
Consistency matters more than timing. Pick a day and approximate time, then stick with it. Your body maintains more stable semaglutide levels when the interval between doses is regular.
Exercise and injection timing
Avoid injecting immediately before or after intense exercise. Physical activity increases blood flow to muscles and can alter absorption dynamics, especially if you inject in the thigh and then go for a run. Wait at least one hour after exercise before injecting, or inject in a body area you will not be heavily using during your workout.
Comparing semaglutide injection sites to other GLP-1 medications
If you are curious how semaglutide injection site considerations compare to other medications in the same class, the principles are remarkably consistent. GLP-1 injection site guidelines apply broadly to the entire medication category because they all use the subcutaneous delivery route.
Tirzepatide follows the same three-site system: abdomen, thigh, and upper arm. The rotation principles are identical. The absorption differences between sites are comparable. If you ever switch between tirzepatide and semaglutide or convert your dose from one to the other, your injection site habits can carry over directly.
Retatrutide, the newer triple-agonist peptide, also uses subcutaneous injection with the same site options. The retatrutide injection guide mirrors semaglutide injection recommendations almost exactly. The fundamentals of subcutaneous injection do not change based on the specific medication. What changes is the dose, the frequency, and the concentration, not the injection technique.
For users managing multiple peptide protocols, consistent injection habits across all medications simplify the process enormously. Use the same rotation schedule, the same technique, and the same tracking method for every subcutaneous injection in your regimen.
What the research actually shows
Let us look at what clinical studies and prescribing data tell us about injection site significance. The evidence base is clear, even if internet forums make it sound controversial.
Novo Nordisk conducted pharmacokinetic studies during semaglutide development that compared absorption across injection sites. The conclusion in the prescribing information is unambiguous: "similar exposure" is achieved regardless of which approved site is used. This language was reviewed and accepted by the FDA.
A study published in the journal Clinical Therapeutics compared the injection-site experience of semaglutide in single-dose and multi-dose pen injectors. The researchers found that injection site pain scores were generally low across all sites, with no significant difference in patient comfort between the abdomen, thigh, and upper arm when proper technique was used.
The broader literature on subcutaneous injection pharmacokinetics shows that absorption rate differences between sites are a function of tissue blood flow and fat composition. These differences are predictable, consistent, and accounted for in the medication dose and formulation. Drug manufacturers design subcutaneous medications knowing that patients will use different injection sites, and they ensure the therapeutic window is wide enough to accommodate these normal variations.
The strongest evidence supporting injection site significance relates to complications from poor rotation, not from site selection itself. Studies on lipohypertrophy in insulin-dependent diabetic patients (who inject far more frequently than once-weekly semaglutide users) consistently show that tissue damage from repeated injection in the same site causes clinically meaningful absorption problems. These findings translate directly to semaglutide users, particularly those on long-term protocols who inject in the same spot week after week.
When injection site problems signal something bigger
Most injection site issues are localized and temporary. But occasionally, reactions at the injection site indicate a more significant concern that warrants medical attention.
Allergic reactions: True allergic reactions to semaglutide are rare but possible. Signs include widespread hives (not just at the injection site), difficulty breathing, swelling of the face or throat, rapid heartbeat, or severe dizziness. These require immediate emergency medical attention. A localized red bump at the injection site is not an allergic reaction. A spreading rash that extends well beyond the injection area might be.
Persistent nodules: Small nodules that resolve within days are normal. Hard lumps that persist for weeks, grow larger, or become painful should be evaluated. They may indicate lipohypertrophy, abscess formation, or granuloma reaction to the injected material.
Infection signs: Increasing redness, warmth, swelling, and tenderness over 24-48 hours after injection, especially if accompanied by fever or pus at the site, suggest infection. This is uncommon with proper hygiene but requires antibiotic treatment. Do not inject into or near an infected area until it has fully healed.
Skin changes: If you notice unusual skin sensitivity with semaglutide, persistent discoloration, or textural changes at injection sites, discuss these with your provider. Some users experience allodynia (heightened skin sensitivity) as a systemic side effect of semaglutide that manifests most noticeably at injection areas.
Practical tools for managing injection sites
Successful long-term semaglutide use requires a system, not just knowledge. Here are practical tools and strategies that help you maintain proper injection habits consistently.
Body maps: Print or draw a simple outline of the front and back of your body. Mark each injection with the date and a small dot at the exact location. Over weeks and months, this visual record shows you exactly which areas are overused and which have been resting.
Phone reminders: Set your weekly injection reminder to include a note about which body zone to use next. "Wednesday 8pm - LEFT THIGH" takes the decision-making out of the process and ensures you follow your rotation schedule.
The SeekPeptides semaglutide dosage calculator helps you determine your exact dose, and pairing that precision with proper injection site management ensures every microgram reaches your system as intended. When the dose is right and the technique is right, the results follow.
For broader injection guidance and peptide injection best practices, SeekPeptides offers comprehensive guides that cover every aspect of subcutaneous administration, from reconstitution to storage after reconstitution to safety protocols.
Putting it all together: a complete injection site protocol
Here is a step-by-step protocol that incorporates everything in this guide into a practical weekly routine.
Step 1: Check your rotation log. Which body zone is next? Move to that area. Never inject in the same zone you used last week.
Step 2: Warm the medication. Remove semaglutide from the refrigerator 15-30 minutes before injection. Room-temperature medication reduces discomfort significantly.
Step 3: Select your exact spot. Within your chosen body zone, pick a specific point at least one inch from any previous injection site. Avoid scars, moles, veins, stretch marks, and previously irritated areas.
Step 4: Clean the site. Wipe the area with an alcohol swab in a circular motion from center outward. Allow the alcohol to dry completely, typically 15-20 seconds.
Step 5: Prepare the skin. If needed (lean users, thigh or arm injections), pinch a fold of skin and fat. Hold this pinch throughout the injection.
Step 6: Insert the needle. At a 90-degree angle, push the needle all the way in with a quick, smooth motion. Hesitating makes it more painful.
Step 7: Inject the dose. Press the pen button or depress the syringe plunger steadily. Do not rush.
Step 8: Hold for 10 seconds. Keep the needle in place. Count to ten. This ensures complete dose delivery.
Step 9: Withdraw the needle. Pull straight out at the same angle you inserted. Apply gentle pressure with a cotton ball if needed. Do not rub.
Step 10: Log the injection. Record the date, body zone, exact location, and any notes (pain level, reaction, dose). Update your rotation schedule for next week.
This process takes less than five minutes and becomes automatic after a few weeks. The discipline pays off in consistent results, minimal complications, and a comfortable injection experience that you can maintain for as long as your semaglutide protocol continues.
Frequently asked questions
Does injecting semaglutide in the stomach work better than the thigh?
The abdomen absorbs semaglutide slightly faster due to higher blood flow, but this does not translate to meaningfully better weight loss or appetite suppression. The FDA considers all three approved sites equivalent. Choose based on comfort and rotate consistently for optimal long-term results.
Can I inject semaglutide in my buttocks?
The buttocks are not an FDA-approved injection site for semaglutide. Stick to the abdomen, thigh, or upper arm. Using unapproved sites risks unpredictable absorption and has not been studied for safety or efficacy with this medication.
What happens if I inject semaglutide in the wrong spot?
If you inject into an approved area but in a suboptimal location (near a scar, too close to the navel, in a previously used spot), the medication will still absorb. You may experience more discomfort or slightly inconsistent absorption, but one imperfect injection will not derail your progress. Correct the issue for your next dose.
How far apart should injection sites be from each other?
At minimum, one inch (2.5 cm) from your previous injection site. Ideally, use a completely different body zone each week. Greater distance between consecutive injections gives tissue more recovery time and reduces the risk of lipohypertrophy.
Should I change my injection site if semaglutide stops working?
If you have been injecting in the same spot repeatedly and notice reduced effectiveness, tissue damage at that site may be contributing to absorption problems. Switch to a different body zone and implement proper rotation. If effectiveness does not improve, discuss dose adjustment with your provider.
Is it normal for the injection site to itch?
Mild itching at the injection site is common and usually resolves within hours. It is a minor histamine response to the needle and medication. Over-the-counter antihistamine cream can provide relief. Intense or widespread itching that extends beyond the injection area should be reported to your healthcare provider.
Can I inject semaglutide in an area with stretch marks?
It is best to avoid areas with heavy stretch marks because the tissue structure is altered and absorption may be inconsistent. Light stretch marks are less of a concern. When in doubt, choose a clear area of skin for the most reliable medication delivery.
Does ice before injection help with pain?
Applying ice for 1-2 minutes before injection can numb the area and reduce needle insertion pain. Some users swear by this technique, while others find that the cold causes the skin to tense up and makes the injection harder. Experiment to see what works for your body. Just be sure to clean the area with alcohol after removing the ice.
External resources
PMC: Comparison of injection-site experience of semaglutide pen injectors
PMC: Injection-site nodules associated with subcutaneous semaglutide
For researchers serious about optimizing their semaglutide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions. Members access detailed semaglutide optimization strategies, dosage calculators, and expert guidance for every stage of the journey.
In case I do not see you, good afternoon, good evening, and good night. May your injection sites stay healthy, your rotation stay consistent, and your results stay on track.