Apr 4, 2026

You started tirzepatide expecting nausea, maybe some appetite changes, possibly fatigue. Nobody warned you about the bathroom trips. Yet here you are, up twice at night, mapping out restroom locations before errands, wondering if something is wrong. You are not imagining it. And you are not alone.
The strange part? Frequent urination is not listed as an official side effect on the tirzepatide prescribing information. Clinical trials focused on nausea, diarrhea, and decreased appetite. Urinary changes did not make the cut. But thousands of users report it, and the reasons are more complex than most guides acknowledge. Some of those reasons are temporary and harmless. Others deserve medical attention. Knowing the difference matters.
This guide breaks down every mechanism behind increased urination on tirzepatide, from glycogen depletion to renal tubule changes to blood sugar normalization. We will cover what the research actually says about GLP-1 receptor agonists and kidney function, which concurrent medications amplify the effect, and exactly what to do about it. Whether you are dealing with mild inconvenience or something that disrupts your sleep, you will find specific, actionable answers here.
SeekPeptides members often ask about unexpected side effects like this one, and understanding why your body responds the way it does is the first step toward managing it effectively.
Is increased urination a real side effect of tirzepatide?
Let us start with the facts. The SURPASS clinical trial program, which evaluated tirzepatide in over 6,000 patients with type 2 diabetes, did not identify frequent urination as a statistically significant adverse event. The SURMOUNT trials for weight management told the same story. Polyuria and urinary frequency did not appear at rates meaningfully different from placebo.
So does that mean it does not happen? Not at all.
Clinical trials track predefined adverse events with strict reporting criteria. If a side effect is not specifically monitored or falls below a certain reporting threshold, it can slip through the data net entirely. What clinical trials miss, patient experience reveals. And the patient experience is clear: many people on tirzepatide notice they are peeing more, especially in the first several weeks of treatment.
The distinction matters. Increased urination is likely not a direct pharmacological effect of tirzepatide in the way that nausea or diarrhea are. Instead, it results from a cascade of indirect changes that tirzepatide triggers in your body, including metabolic shifts, fluid redistribution, dietary changes, and improved blood sugar regulation. Each of these deserves its own explanation because each requires a different response.
Glycogen depletion and water release
This is the most common reason for increased urination in the first few weeks on tirzepatide. It is also the most temporary.
Your body stores glucose as glycogen in your liver and muscles. Here is the important part: every gram of glycogen binds approximately 3 grams of water. When tirzepatide reduces your appetite and caloric intake drops, your body starts burning through those glycogen stores for energy. As glycogen depletes, the water bound to it releases into your bloodstream. Your kidneys filter that excess water. You pee it out.
The math is straightforward. An average person stores 400 to 500 grams of glycogen. That means roughly 1,200 to 1,500 grams of water, about 2.5 to 3.3 pounds, can release as glycogen stores deplete. This is why early weight loss on tirzepatide often seems dramatic. Much of it is water.
This process typically peaks during weeks one through three. Some people experience it as noticeably increased urination frequency. Others barely notice. The intensity depends on how much your caloric intake drops, how large your glycogen stores were to begin with, and how your kidneys handle the fluid shift.
The good news? It resolves on its own. Once your glycogen stores reach a new equilibrium at your reduced caloric intake, the excess water release stops. Most people find that the dramatic bathroom frequency settles down by week four to six.
How to manage glycogen-related urination
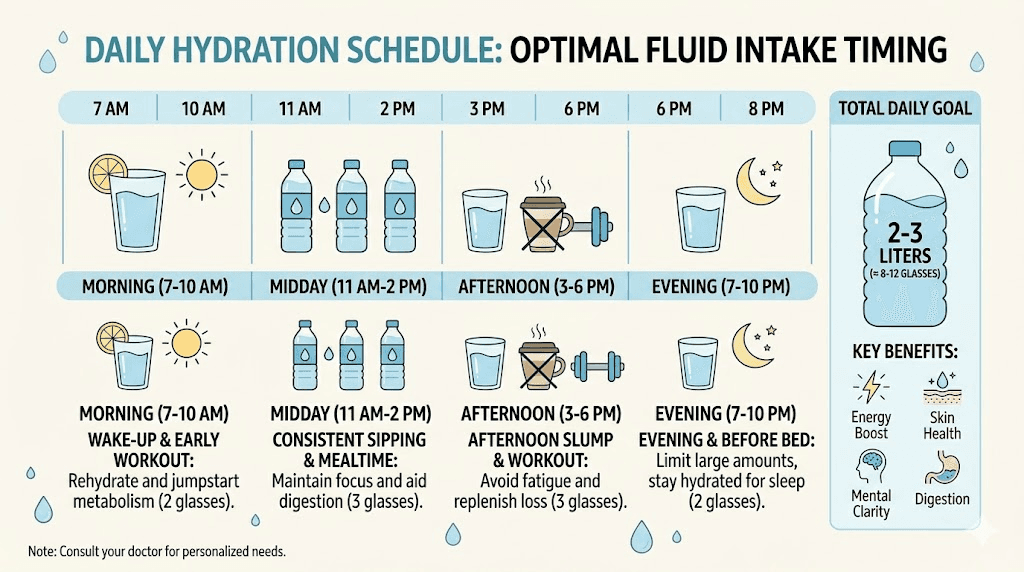
Do not restrict fluids to compensate. This is a common mistake. Your body is losing water it does not need, but restricting fluids can push you toward dehydration, which creates far worse problems. Instead, maintain steady hydration throughout the day, aiming for clear to pale yellow urine as your target color. Front-load your fluid intake earlier in the day if nighttime urination is disrupting sleep, and reduce intake two to three hours before bedtime.
Electrolytes matter here too. When you excrete excess water, you lose sodium, potassium, and magnesium along with it. Electrolyte supplementation or mineral-rich foods can prevent the cramping, fatigue, and dizziness that sometimes accompany this phase.
Blood sugar normalization and osmotic changes
If you are using tirzepatide for type 2 diabetes management, the urination picture gets more nuanced.
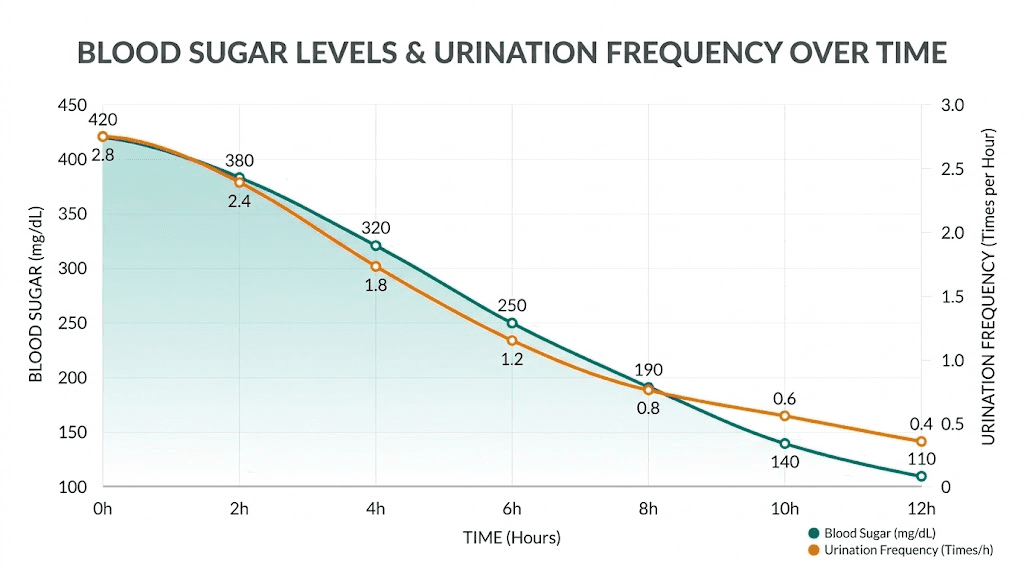
High blood sugar causes something called osmotic diuresis. When glucose levels exceed your kidneys reabsorption capacity (roughly 180 mg/dL), glucose spills into your urine. Water follows glucose. This is why frequent urination and excessive thirst are classic symptoms of uncontrolled diabetes.
Now here is the counterintuitive part. When tirzepatide improves your blood sugar control, osmotic diuresis should decrease. Less glucose spilling into urine means less water following it. For many diabetic patients, tirzepatide actually reduces urinary frequency over time.
But the transition period can be confusing. As your blood sugar drops from chronically elevated levels to a normal range, your body undergoes fluid redistribution. Tissues that were retaining water due to high glucose begin releasing it. Your kidneys adjust their filtration rate. During this recalibration, which can last several weeks, urinary patterns fluctuate unpredictably.
Some people notice increased urination right as their blood sugar normalizes, followed by a gradual return to normal bathroom frequency. Others experience the opposite, decreased frequency that then stabilizes. The trajectory depends on how elevated your glucose was before starting treatment and how quickly tirzepatide brings it down.
Monitoring during the transition
If you have diabetes or prediabetes, tracking your blood sugar alongside your urinary frequency provides valuable context. A pattern where urination increases as blood sugar drops is typically benign, it is your body adjusting to better glucose control. A pattern where urination increases alongside rising blood sugar is a red flag that demands immediate medical attention.
Keep a simple log for one to two weeks after starting tirzepatide or increasing your dose. Note your dosage, blood sugar readings, fluid intake, and bathroom frequency. This data helps your healthcare provider distinguish between harmless adjustment and something requiring intervention.
The GLP-1 receptor and kidney function
Tirzepatide is a dual GIP/GLP-1 receptor agonist. The GLP-1 component has direct effects on kidney function that most patient-facing resources completely ignore. Understanding this mechanism helps explain why some degree of urinary change might be pharmacologically driven, even if clinical trials did not flag it as a common side effect.
Research published in the American Journal of Physiology demonstrates that GLP-1 receptor activation in the kidneys inhibits the sodium/hydrogen exchanger isoform 3 (NHE3) in the proximal tubule. NHE3 normally reabsorbs sodium, bicarbonate, and water from the filtrate back into your blood. When GLP-1 receptor agonists inhibit NHE3, less sodium gets reabsorbed. Water follows sodium. More water ends up in your urine.
The pathway works like this. GLP-1 receptor activation increases intracellular cyclic AMP (cAMP). This activates protein kinase A (PKA), which phosphorylates NHE3 at specific sites (serines 552 and 605). Phosphorylated NHE3 moves less sodium. Less sodium reabsorption means less water reabsorption. The result is a mild natriuretic and diuretic effect.
This is not dramatic enough to cause clinical dehydration in most people. But it contributes to the overall picture, especially when combined with glycogen water release and dietary changes. Think of it as one factor among several, each individually small, but collectively noticeable.
There is a positive angle to this mechanism. GLP-1 mediated natriuresis may contribute to the blood pressure reductions observed with tirzepatide. Less sodium retention means lower blood volume means lower blood pressure. The kidney effect that makes you pee a bit more might also be protecting your cardiovascular system.
What the renal safety data shows
A systematic review and meta-analysis published in the World Journal of Diabetes examined tirzepatide renal safety data across multiple trials. The findings were reassuring. Tirzepatide did not increase risks of adverse renal events, urinary tract infections, nephrolithiasis (kidney stones), acute kidney injury, or renal cancer compared to placebo, insulin, or other GLP-1 receptor agonists.
Even more encouraging, tirzepatide was associated with reduced urine albumin-to-creatinine ratio (UACR) after 24 weeks, sustained through week 72, without detrimental changes to estimated glomerular filtration rate (eGFR). In the pooled SURPASS trials, the adjusted mean percent change from baseline in UACR for tirzepatide 5, 10, and 15 mg compared with all comparators was minus 19.3%, minus 22.0%, and minus 26.3% respectively at week 40 to 42.
Translation: tirzepatide appears to be protective of kidney function, not harmful. If you are peeing more on tirzepatide, the medication is almost certainly not damaging your kidneys. If anything, it may be helping them.
Concurrent medications that amplify urination
This is a factor that many people overlook entirely. If you are taking other medications alongside tirzepatide, some of them may be the real driver behind your increased bathroom visits.
SGLT2 inhibitors
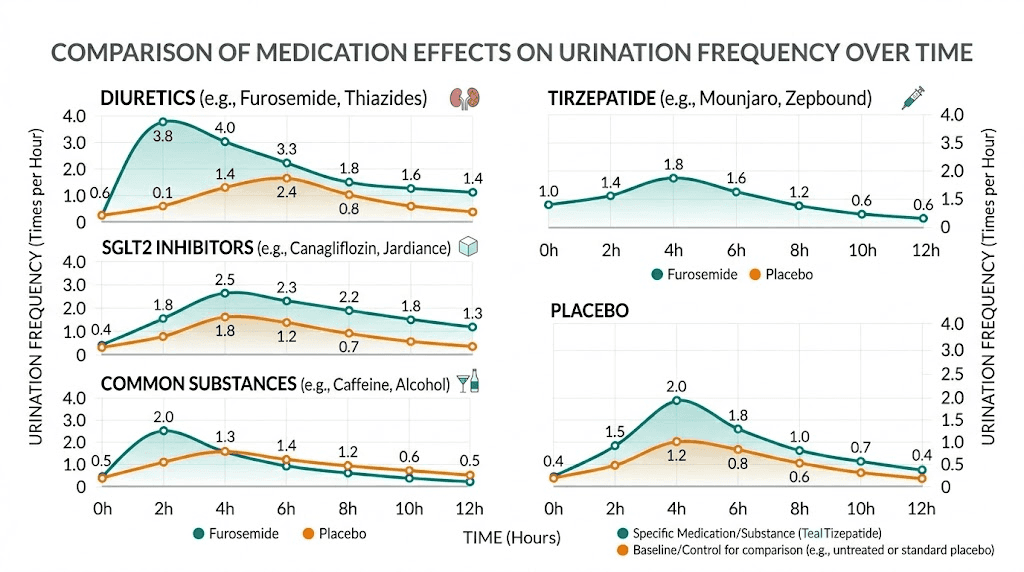
Medications like empagliflozin (Jardiance), dapagliflozin (Farxiga), and canagliflozin (Invokana) work by intentionally increasing glucose excretion through urine. They block glucose reabsorption in the kidneys. Glucose pulls water with it. If you take an SGLT2 inhibitor alongside tirzepatide, you will almost certainly notice more frequent urination, and it is the SGLT2 inhibitor doing most of the work.
This combination is common in diabetes management, and the increased urination is an expected, intended therapeutic effect. But patients sometimes attribute it entirely to the newer medication (tirzepatide) when the SGLT2 inhibitor has been causing it all along.
Diuretics
Thiazide diuretics (hydrochlorothiazide), loop diuretics (furosemide), and potassium-sparing diuretics (spironolactone) all increase urine output by design. If you take any of these for blood pressure management or edema, they are a significant contributor to your bathroom frequency. As tirzepatide produces weight loss and potentially lowers blood pressure on its own, your provider may consider adjusting or discontinuing your diuretic. This conversation is worth having.
Metformin
Metformin and tirzepatide together is a common combination. Metformin itself can affect kidney function and fluid balance, though its urinary effects are modest compared to SGLT2 inhibitors or diuretics. Still, it adds to the cumulative picture.
Caffeine and alcohol
Not medications per se, but worth mentioning. Both caffeine and alcohol are diuretics. If your tirzepatide regimen coincides with increased coffee intake (common when appetite decreases and people substitute meals with coffee) or social drinking, the combined effect on urination can be substantial.
Dietary changes and fluid intake shifts
Tirzepatide changes what you eat. That changes how much you pee. The connection is more direct than most people realize.
When appetite decreases, people naturally gravitate toward lighter, more hydrating foods. Soups, smoothies, fruits, salads. All of these have high water content. Meanwhile, dense, dry foods like bread, rice, and pasta, which absorb water during digestion, become less appealing. The net effect is more water entering your system through food even if you are not consciously drinking more.
Then there is the deliberate increase in fluid intake. Every tirzepatide diet guide emphasizes staying hydrated. Every healthcare provider recommends it. Many people increase their water intake from four to five glasses daily to eight or ten. That alone can double your urinary output.
Additionally, high-protein diets, which are commonly recommended while on tirzepatide to preserve muscle mass, generate more urea as a metabolic byproduct. Urea acts as an osmotic agent in the kidneys, pulling water into urine. More protein means more urea means slightly more urine production.
The nausea-hydration cycle
Here is a pattern nobody talks about. Tirzepatide causes nausea in a significant percentage of users, especially during the early dose escalation phase. The standard advice for managing nausea? Sip water frequently. Eat smaller meals. Choose bland, hydrating foods.
So tirzepatide causes nausea. Nausea management increases fluid intake. Increased fluid intake causes more urination. The medication is not directly causing the urination, but it is creating the conditions that lead to it. Recognizing this cycle helps you understand that the solution is not less water, it is strategic timing of your fluid intake.
When increased urination is a warning sign
Most urinary changes on tirzepatide are benign and temporary. But some patterns demand immediate attention. Knowing the difference could save your life.
Signs that require urgent medical attention
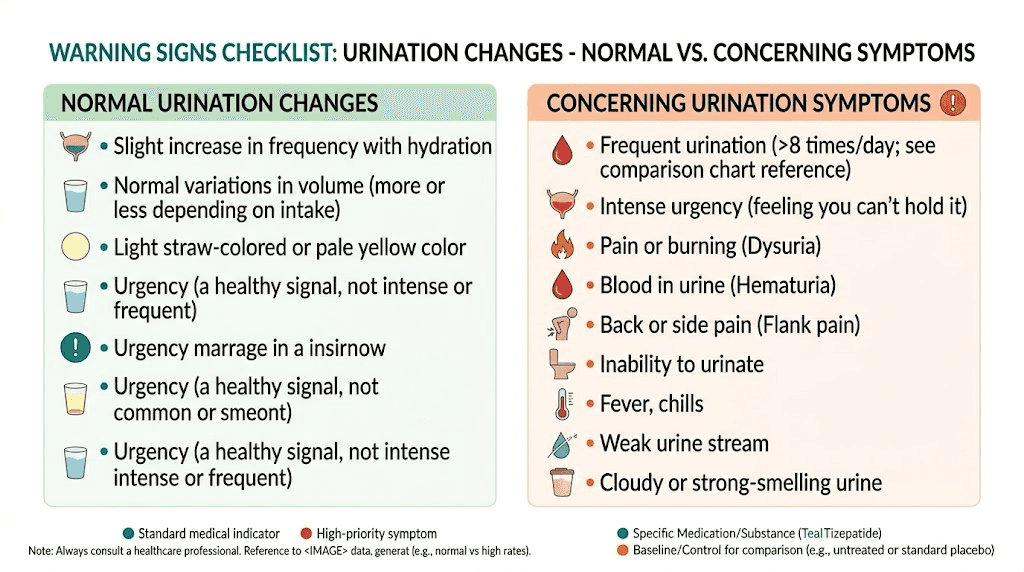
Excessive thirst combined with massive urine output. If you are drinking constantly and still feel parched, and producing large volumes of dilute urine, this could signal a blood sugar emergency. While tirzepatide typically improves glucose control, dose adjustments or missed doses can cause glucose spikes. Diabetic ketoacidosis (DKA) presents with extreme thirst, frequent urination, nausea, abdominal pain, and fruity-smelling breath. This is a medical emergency.
Dark, concentrated urine despite adequate fluid intake. This suggests your kidneys are not filtering properly. While tirzepatide is generally kidney-protective, severe gastrointestinal side effects (persistent vomiting, diarrhea) can cause dehydration that stresses kidney function. If your urine is consistently dark amber despite drinking plenty of fluids, contact your provider.
Pain, burning, or blood during urination. These suggest urinary tract infection (UTI) or other genitourinary issues unrelated to tirzepatide. While clinical data shows tirzepatide does not increase UTI risk, UTIs can occur coincidentally and need treatment.
Sudden decrease in urine output. This is more concerning than increased urination. If you suddenly stop urinating normally despite adequate fluid intake, it could indicate acute kidney injury. Seek medical attention immediately.
Swelling in legs, feet, or face alongside urinary changes. Fluid retention combined with altered urination can signal kidney problems or heart failure. Neither is common with tirzepatide, but both require evaluation.
Signs that are probably fine
Mild increase in urination frequency during the first four to six weeks, especially if accompanied by early weight loss. This is almost certainly glycogen water release and will resolve. Slightly more frequent urination that correlates with increased fluid intake. Basic math, more water in means more water out. Nighttime urination once or twice if you are drinking fluids close to bedtime. Adjust your timing, not your total intake.
Practical strategies for managing frequent urination
Knowing why you are peeing more is useful. Knowing what to do about it is essential. Here are specific, tested approaches organized by the underlying cause.
Strategy 1: Front-load your hydration
Drink the majority of your daily fluids before 4 pm. This means loading up on water in the morning and early afternoon, then tapering intake in the evening. You still get adequate hydration. You just shift the resulting urination to daytime hours when it is less disruptive. Aim to consume roughly 70% of your daily fluids before dinner. Cut off fluid intake two to three hours before bedtime entirely, except small sips if needed with medications.
Strategy 2: Replace electrolytes proactively
Increased urination means increased electrolyte loss. Sodium, potassium, and magnesium all leave your body with urine. Without replacement, you can develop muscle cramps, leg cramps, dizziness, fatigue, and headaches. These symptoms often get blamed on tirzepatide itself when they are actually electrolyte depletion from increased urination.
Quality electrolyte supplements designed for people on GLP-1 medications can help. Look for products containing sodium, potassium, and magnesium in balanced ratios. Avoid those loaded with sugar. Alternatively, bone broth, mineral water, and adding a pinch of salt to meals can help maintain electrolyte balance naturally.
Strategy 3: Time your tirzepatide injection strategically
While there is no definitive evidence that injection timing affects urination patterns, some users report that taking their weekly tirzepatide injection in the morning rather than evening helps minimize nighttime bathroom disruption. The logic is that any acute metabolic effects peak during waking hours rather than during sleep. It is worth experimenting with if nocturia is your primary complaint.
Strategy 4: Review your complete medication list
Make a list of every medication, supplement, and regular beverage in your daily routine. Circle anything with diuretic properties: SGLT2 inhibitors, thiazide or loop diuretics, caffeine, alcohol, certain herbal teas (dandelion, nettle, parsley). Share this list with your prescribing provider. They may be able to adjust timing, reduce dosages, or eliminate medications that are no longer necessary as tirzepatide takes effect.
This is especially important for blood pressure medications. As tirzepatide produces weight loss, many patients experience natural blood pressure improvements. Diuretics and antihypertensives may need dose reductions. Continuing them at full strength while tirzepatide is also lowering blood pressure can create excessive fluid loss.
Strategy 5: Strengthen your pelvic floor
If the issue is not frequency alone but also urgency, the feeling that you cannot hold it, pelvic floor exercises can help. Kegel exercises strengthen the muscles that control urination. Both men and women can benefit. Start with three sets of ten repetitions daily, holding each contraction for five seconds. Increase duration over time.
Weight loss itself can improve urinary urgency and incontinence, especially in women. Excess abdominal weight puts pressure on the bladder. As tirzepatide helps reduce that weight, bladder symptoms often improve naturally over months. One study found that a 5% to 10% reduction in body weight significantly reduced stress urinary incontinence episodes in obese women.
Strategy 6: Practice timed voiding
Rather than waiting until your bladder feels full, establish a regular bathroom schedule. Go every two to three hours during waking hours, whether you feel the urge or not. This trains your bladder to function on a predictable schedule and reduces urgency episodes. It also prevents overfilling, which can stretch the bladder wall and worsen frequency over time.
How urination patterns change over time on tirzepatide
Understanding the typical timeline helps set realistic expectations and reduces anxiety about whether something is wrong.
Weeks 1 through 3: The adjustment phase
This is when urinary changes are most noticeable. Glycogen stores are depleting, fluid is redistributing, your diet is shifting, and your body is adjusting to the medication. Some people report three to five additional bathroom trips per day during this phase. Nighttime urination is common. This is normal.
Weeks 4 through 8: Stabilization begins
As glycogen reaches a new equilibrium, the dramatic water release subsides. Blood sugar levels, if previously elevated, begin stabilizing at their new lower range. Dietary patterns settle into routines. Most people notice a significant decrease in bathroom frequency compared to the first few weeks. You may still be going slightly more often than before tirzepatide, but it is no longer disruptive.
Weeks 8 through 12: New normal
By this point, your body has largely adapted. Any ongoing increase in urination is likely due to sustained factors like higher fluid intake, dietary changes, or concurrent medications rather than acute metabolic shifts. If urination has not normalized by week 12, that is a strong signal to discuss it with your healthcare provider and investigate non-tirzepatide causes.
Dose escalation resets
One thing to know: dose increases can temporarily restart some of these patterns. Moving from 2.5 mg to 5 mg, or from 5 mg to 10 mg, can trigger a new round of appetite suppression, caloric reduction, and glycogen depletion. The urinary effects of dose escalation are typically milder and shorter-lived than the initial adjustment, but they can catch people off guard if they thought the bathroom trips were behind them.
Tirzepatide, kidneys, and long-term safety
If you are peeing more, a natural concern is whether tirzepatide is harming your kidneys. The research is not just reassuring. It is actively encouraging.
A pooled post hoc analysis of the SURPASS-1 through SURPASS-5 clinical trials published in Diabetes Care found that tirzepatide was associated with significant reductions in albuminuria, a key marker of kidney damage. The UACR reductions were dose-dependent, larger at higher doses, and sustained through 72 weeks of treatment without any detrimental effect on estimated glomerular filtration rate.
Separate research comparing tirzepatide to dulaglutide in patients with high-risk chronic kidney disease and type 2 diabetes found that tirzepatide may reduce risks for kidney function decline, albuminuria increases, and composite major kidney events.
The Cardiology Advisor reported findings that tirzepatide slows kidney decline even in people with prediabetes and overweight or obesity, not just established diabetes. This suggests the kidney-protective effects are not solely driven by blood sugar improvements but may involve direct renal mechanisms.
Bottom line: peeing more on tirzepatide does not mean your kidneys are struggling. Available evidence strongly suggests the opposite, that tirzepatide is actively supporting kidney health through multiple pathways including reduced inflammation, improved metabolic function, and decreased albuminuria.
Special considerations for specific populations
Women
Women are more susceptible to urinary frequency changes for several reasons. Anatomically shorter urethras mean bladder infections are more common. Hormonal fluctuations, including those that occur with significant weight loss, can affect bladder muscle tone. Pelvic floor weakness from pregnancy or aging amplifies urgency symptoms. If you are a woman experiencing significant urinary changes on tirzepatide, mention it to your provider. Tirzepatide can affect hormonal balance in ways that indirectly influence bladder function.
People with existing kidney conditions
If you have chronic kidney disease (CKD), any change in urination warrants closer monitoring. The research on tirzepatide in CKD patients is encouraging, showing kidney-protective effects, but individual responses vary. Your nephrologist should be involved in managing your tirzepatide therapy, and regular eGFR and UACR monitoring is essential.
Older adults
Age-related changes in kidney function, bladder capacity, and prostate health (in men) all affect urination independently. Adding tirzepatide to this mix requires careful attention. Dehydration risk is higher in older adults because thirst sensation diminishes with age. If you are over 65 and experiencing increased urination on tirzepatide, proactive hydration and electrolyte management become even more important. Talk to your provider about whether any of your current medications can be adjusted.
People taking tirzepatide for weight loss without diabetes
Your experience may differ from diabetic patients because you are not dealing with blood sugar normalization as a variable. For you, increased urination is most likely driven by glycogen depletion, dietary changes, and increased fluid intake. The timeline to resolution is typically shorter because there are fewer metabolic factors in play. Expect the most significant changes during weeks one through four, with substantial improvement by week six to eight.
The connection between tirzepatide, UTIs, and urinary health
A common concern is whether tirzepatide increases your risk of urinary tract infections. The clinical data is clear: it does not.
The systematic review of tirzepatide renal safety data found no increased risk of UTIs compared to placebo, insulin, or GLP-1 receptor agonists. This distinguishes tirzepatide from SGLT2 inhibitors, which do carry an elevated UTI risk because they increase glucose in urine, providing a growth medium for bacteria.
Tirzepatide may actually reduce UTI risk in diabetic patients by improving blood sugar control. Less glucose in urine means less fuel for bacterial growth. This is one of the indirect benefits of improved glycemic management.
That said, if you experience UTI symptoms, burning during urination, cloudy or foul-smelling urine, pelvic pain, or fever, do not assume it is just a tirzepatide side effect. UTIs require antibiotic treatment regardless of what medications you are taking.
Nighttime urination (nocturia): the most disruptive symptom
Daytime bathroom frequency is annoying. Nighttime urination is genuinely harmful. Disrupted sleep affects hormones, appetite regulation, mood, immune function, and paradoxically, weight loss itself. Poor sleep can actually slow your progress on tirzepatide.
Nocturia on tirzepatide deserves aggressive management because the downstream effects of sleep disruption undermine the very goals the medication is meant to achieve.
Targeted nocturia management protocol
Step 1: Cut evening fluids. Stop drinking two to three hours before bed. If you take evening medications that require water, use the minimum amount needed.
Step 2: Limit evening diuretics. Caffeine after 2 pm, alcohol in the evening, and certain herbal teas should be moved to earlier in the day or eliminated temporarily.
Step 3: Elevate your legs. If you have any degree of lower extremity edema, elevating your legs for 30 to 60 minutes before bed allows accumulated fluid to redistribute and be excreted before you lie down rather than during the night.
Step 4: Empty your bladder twice before bed. Go to the bathroom as part of your bedtime routine. Then wait 15 to 20 minutes and go again. This double-void technique ensures your bladder is as empty as possible before sleep.
Step 5: Adjust injection timing. If you inject tirzepatide in the evening, try switching to morning injection to see if nighttime urination improves. Give this change at least two to three weeks before evaluating.
Step 6: Track and report. If nocturia persists beyond six weeks despite these interventions, bring your tracking log to your healthcare provider. Persistent nocturia may have causes unrelated to tirzepatide that need investigation, including prostate enlargement in men, overactive bladder, or sleep apnea.
Comparing urinary effects across GLP-1 medications
If you switched to tirzepatide from another GLP-1 medication like semaglutide, you may wonder whether the urinary effects are specific to tirzepatide or common across the class.
The answer is that increased urination is reported across all GLP-1 receptor agonists, not just tirzepatide. The NHE3 inhibition mechanism in the renal proximal tubule is a class-wide effect tied to GLP-1 receptor activation. The indirect causes, glycogen depletion, dietary changes, blood sugar normalization, are also shared across medications that produce significant weight loss and metabolic improvement.
Tirzepatide, as a dual GIP/GLP-1 agonist, may produce slightly more pronounced effects because it typically produces greater weight loss (15% to 20% of body weight versus 10% to 15% for pure GLP-1 agonists) and more dramatic metabolic improvements. More weight loss means more glycogen depletion means more water release. But the fundamental mechanisms are the same.
Medication | Class | Average weight loss | Reported urinary changes | Mechanism |
|---|---|---|---|---|
Tirzepatide | Dual GIP/GLP-1 | 15-20% | Moderate, weeks 1-6 | NHE3 inhibition + glycogen + dietary |
Semaglutide | GLP-1 | 10-15% | Mild-moderate, weeks 1-4 | NHE3 inhibition + glycogen + dietary |
Liraglutide | GLP-1 | 5-8% | Mild | NHE3 inhibition + modest glycogen |
Dulaglutide | GLP-1 | 5-10% | Mild | NHE3 inhibition + glycogen |
If urinary changes were tolerable on semaglutide, they will likely be manageable on tirzepatide. If they were problematic on semaglutide, plan proactive management strategies from day one of your tirzepatide transition.
What your healthcare provider needs to know
When discussing urinary changes with your provider, specific details are more useful than vague complaints. Prepare by tracking for one week.
What to record:
Number of bathroom visits per day (daytime and nighttime separately)
Approximate volume (small, moderate, large)
Any pain, burning, urgency, or incontinence
Urine color throughout the day
Total daily fluid intake (type and amount)
Current tirzepatide dose and how long at this dose
All other medications and supplements
Blood sugar readings if applicable
This data allows your provider to quickly distinguish between harmless metabolic adjustment and something requiring investigation. Without it, the conversation often ends with "drink less water and see how it goes," which is not always the right advice.
SeekPeptides members benefit from comprehensive side effect management guides that help them have more productive conversations with their healthcare providers, turning vague concerns into specific, actionable discussions.
Frequently asked questions
Does tirzepatide directly cause frequent urination?
Tirzepatide does not directly cause frequent urination as a primary pharmacological effect. It is not listed as a common side effect in clinical trial data. However, the metabolic changes it triggers, including glycogen depletion, blood sugar normalization, and dietary shifts, can indirectly increase urination frequency. GLP-1 receptor activation in the kidneys also produces a mild natriuretic effect through NHE3 inhibition in the proximal tubule.
How long does increased urination last on tirzepatide?
For most people, the most noticeable urinary changes occur during weeks one through three and improve significantly by weeks four through six. By week eight to twelve, urination patterns typically stabilize at a new baseline. Dose escalations can temporarily restart the pattern, but subsequent adjustments are usually milder and shorter-lived than the initial experience.
Should I drink less water if I am peeing too much on tirzepatide?
No. Restricting fluid intake while your body is actively losing water through glycogen depletion and metabolic changes increases your dehydration risk. Instead of drinking less, time your intake strategically. Consume most fluids before 4 pm and reduce intake two to three hours before bedtime. Aim for pale yellow urine as your hydration target.
Can tirzepatide damage your kidneys?
Current evidence indicates tirzepatide is kidney-protective, not harmful. Clinical trial data shows reduced albumin-to-creatinine ratios and no increased risk of adverse renal events, acute kidney injury, or kidney stones. Research suggests tirzepatide may even slow kidney function decline in certain populations.
Does tirzepatide increase UTI risk?
No. Unlike SGLT2 inhibitors, tirzepatide does not increase glucose in urine and clinical trials found no elevated UTI risk compared to placebo. Tirzepatide may actually reduce UTI risk in diabetic patients by improving glucose control, which decreases urinary glucose that bacteria feed on.
When should I see a doctor about urination changes on tirzepatide?
Seek medical attention if you experience extreme thirst with massive urine output (possible diabetic emergency), dark urine despite adequate fluid intake, pain or burning during urination, blood in urine, sudden decrease in urine output, or if increased urination persists beyond 12 weeks without improvement. Also contact your provider if urinary changes are accompanied by dizziness, confusion, or significant fatigue suggesting dehydration.
Is peeing more on tirzepatide a sign the medication is working?
In many cases, yes. Increased urination during the first few weeks often indicates glycogen depletion and fluid redistribution, which are signs that your body is responding to reduced caloric intake and beginning to burn stored energy. However, do not use urination frequency as a measure of medication effectiveness. Weight loss, appetite changes, and blood sugar improvements are much more reliable indicators.
Will switching from semaglutide to tirzepatide make me pee more?
Possibly, but not dramatically for most people. If you tolerated semaglutide without significant urinary changes, you will likely have a similar experience on tirzepatide. The GLP-1 renal mechanism is the same. Any additional urinary effects would come from tirzepatide typically producing greater weight loss, which means slightly more glycogen depletion and water release.
External resources
NIH: The physiological role of GLP-1 in the regulation of renal function
Diabetes Care: Tirzepatide associated with reduced albuminuria (SURPASS trials)
World Journal of Diabetes: Renal effects and safety of tirzepatide
AJP-Renal: GLP-1 receptor agonist regulation of NHE3 in renal proximal tubule
For researchers serious about understanding and optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your hydration stay balanced, your kidneys stay healthy, and your bathroom trips stay manageable.