Jan 21, 2026

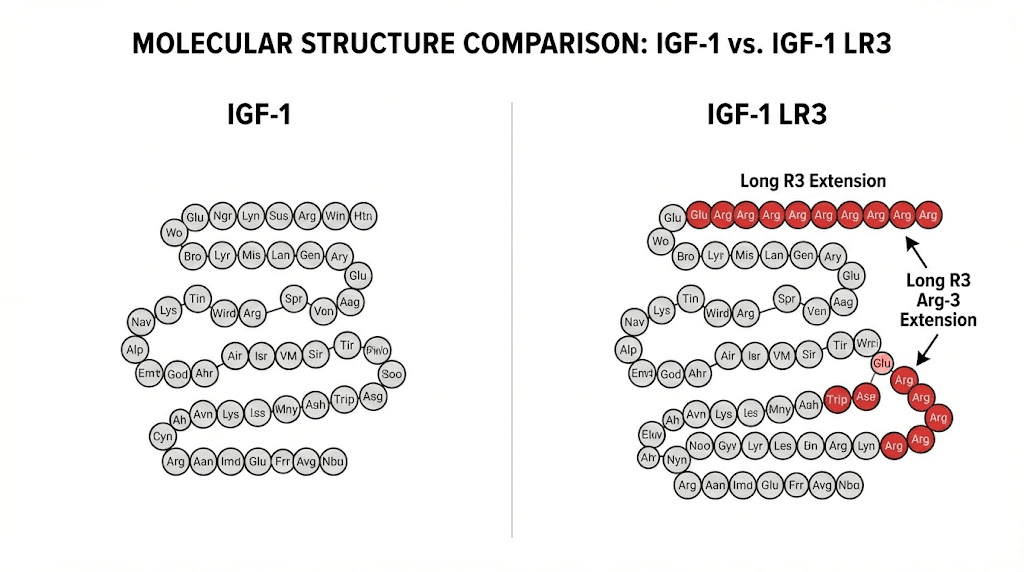
At the molecular level, IGF-1 LR3 represents one of the most significant modifications ever made to a growth factor. Scientists took the 70 amino acid structure of natural IGF-1 and added 13 more at the N-terminus. Then they swapped glutamic acid for arginine at position three. These changes seem small on paper. But they transformed a peptide with a 20-minute half-life into one that circulates for 20 to 30 hours.
That extended activity window changes everything about how the peptide works in the body. Natural IGF-1 gets grabbed almost immediately by binding proteins that shuttle it around and limit its activity. The modified structure of LR3 slips past these binding proteins. It stays active in the bloodstream, reaching tissues throughout the body and exerting its effects for over a full day after each injection.
For researchers interested in peptides for muscle growth, this makes IGF-1 LR3 one of the most potent options available. It doesn't just make existing muscle fibers bigger. It can actually stimulate the creation of new muscle cells, a process called hyperplasia that most compounds simply cannot achieve. This comprehensive guide covers everything you need to know about IGF-1 LR3, from mechanism and dosing to stacking strategies and safety considerations.
SeekPeptides members frequently ask about growth factor peptides because they represent the cutting edge of muscle-building research. Understanding exactly what IGF-1 LR3 does, how it differs from other IGF variants, and how to use it safely requires diving deep into the science.
What is IGF-1 LR3
Long arginine 3-IGF-1, abbreviated as IGF-1 LR3 or LR3-IGF-1, is a synthetic protein and lengthened analogue of human insulin-like growth factor 1. It differs from native IGF-1 in two important ways. First, it possesses an arginine instead of a glutamic acid at the third position in its amino acid sequence. Second, it has an additional 13 amino acids at its N-terminus, bringing the total to 83 amino acids compared to the 70 of standard IGF-1.
These modifications weren't arbitrary. Scientists designed them specifically to overcome the limitations of natural IGF-1. When your liver produces IGF-1 in response to growth hormone, that IGF-1 immediately binds to carrier proteins called insulin-like growth factor-binding proteins. These IGFBPs transport IGF-1 through the bloodstream but also limit its biological activity. Natural IGF-1 has a half-life measured in minutes because of this binding.
The LR3 modifications dramatically reduce binding protein affinity. The result? IGF-1 LR3 retains the pharmacological activity of IGF-1 as an agonist of the IGF-1 receptor while possessing significantly improved metabolic stability. Research indicates it's approximately three times more potent than native IGF-1 with a half-life of about 20 to 30 hours.
For context on where this fits among other IGF peptides, the insulin-like growth factor family includes several variants with different properties and applications.
How IGF-1 LR3 differs from regular IGF-1
The differences between natural IGF-1 and the LR3 variant go beyond half-life. Understanding these distinctions helps explain why researchers choose one over the other.
Natural IGF-1 in its base form is acutely unstable with a half-life under 10 minutes. This makes it impractical for most research applications.
The peptide degrades so quickly that maintaining consistent blood levels would require nearly continuous administration. Most discussions of "IGF-1" in research contexts actually refer to one of the modified variants.
IGF-1 LR3's extended half-life allows for once-daily dosing. The hormone has far greater timeframe to circulate around the body, bind to receptors, and exert its effects. This extended activity makes site-specific injections unnecessary since the peptide will propagate from the injection site throughout the body during its long active window.
The reduced binding protein affinity also means more free IGF-1 LR3 remains available to interact with target tissues. When natural IGF-1 binds to IGFBPs, it's temporarily inactive. LR3 largely bypasses this regulatory system, allowing more direct tissue effects.
IGF-1 LR3 versus IGF-1 DES
Another common IGF-1 variant, IGF-1 DES (Des 1-3), takes the opposite approach to modification. Instead of adding amino acids, DES removes the first three from the N-terminus, creating a truncated 67 amino acid peptide.
This modification results in dramatically different properties. IGF-1 DES has an ultra-short half-life of about 20 to 30 minutes but approximately 10 times the potency at receptor sites compared to native IGF-1. It doesn't circulate systemically like LR3. Instead, it acts locally and degrades quickly.
The practical implications are significant. IGF-1 LR3 works well for systemic, whole-body growth effects with once-daily dosing. IGF-1 DES excels at localized, site-specific applications where researchers inject it directly into target muscles immediately before training. The theory holds that high lactic acid buildup makes IGF-1 receptors more receptive, so injecting into muscles about to be trained maximizes local effects.
For researchers interested in IGF-1 DES sourcing, understanding these differences helps select the right variant for specific research goals.
Feature | IGF-1 LR3 | IGF-1 DES | Natural IGF-1 |
|---|---|---|---|
Amino acids | 83 | 67 | 70 |
Half-life | 20-30 hours | 20-30 minutes | 10-20 minutes |
Potency vs. native | ~3x | ~10x | 1x |
IGFBP binding | Very low | Reduced | High |
Best for | Systemic growth | Localized growth | Reference only |
Injection frequency | Once daily | Multiple daily | Impractical |
How IGF-1 LR3 works in the body
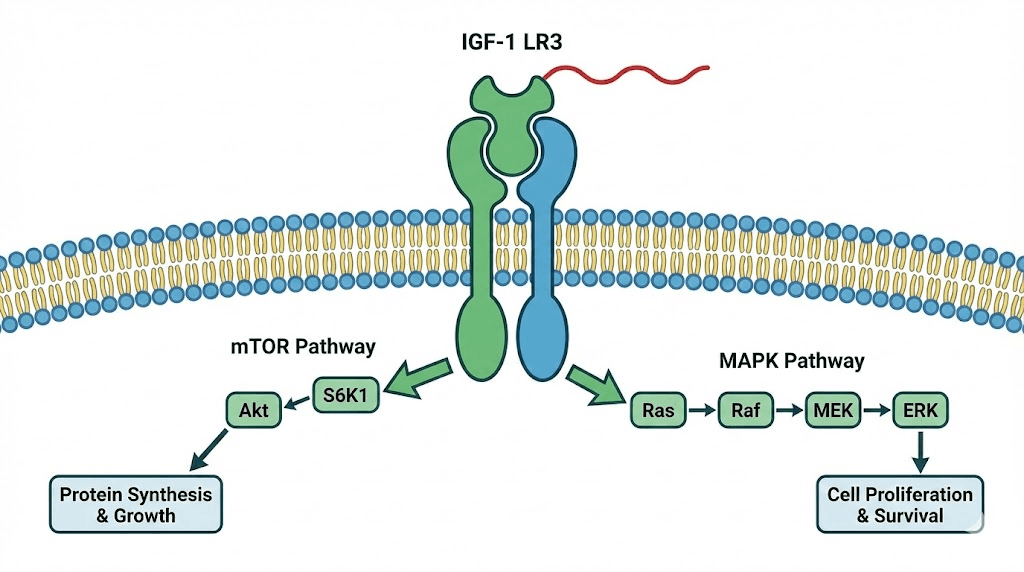
IGF-1 LR3 exerts its effects by binding to the IGF-1 receptor, a transmembrane receptor tyrosine kinase found on virtually every cell type in the body.
This binding activates several intracellular signaling cascades that ultimately drive cell growth, proliferation, and survival.
The two primary pathways activated are the PI3K/Akt/mTOR pathway and the MAPK pathway. The first drives protein synthesis and muscle growth directly. When IGF-1 LR3 binds to its receptor, it triggers a cascade that activates mTOR, the master regulator of protein synthesis in cells. This is the same pathway that resistance training activates, which is why combining IGF-1 LR3 with training can produce synergistic effects.
The MAPK pathway influences cell proliferation and differentiation. This is where IGF-1 LR3's unique ability to stimulate hyperplasia comes from. Most anabolic compounds only cause hypertrophy, making existing muscle fibers larger. IGF-1 LR3 can activate satellite cells, the muscle stem cells responsible for creating entirely new muscle fibers. This represents true muscle cell multiplication rather than just size increase.
Effects on muscle tissue
IGF-1 LR3's muscle-building effects operate through multiple mechanisms simultaneously. Understanding each helps explain why some researchers consider it among the most potent peptides for muscle growth available.
Protein synthesis acceleration: The mTOR activation directly increases the rate at which muscle cells produce new proteins. This accelerated synthesis means faster recovery from training and more efficient conversion of dietary protein into muscle tissue.
Satellite cell activation: Muscle satellite cells normally remain dormant until muscle damage signals them to activate. IGF-1 LR3 directly stimulates these cells even without significant muscle damage. Once activated, satellite cells can fuse with existing muscle fibers to repair them or, in some cases, form entirely new muscle fibers.
Anti-catabolic effects: Beyond building muscle, IGF-1 LR3 helps preserve it. The peptide inhibits protein breakdown pathways, meaning less muscle loss during caloric restriction or periods of reduced training.
Enhanced nutrient delivery: IGF-1 increases blood flow to muscle tissue and improves glucose uptake into muscle cells. This enhanced nutrient delivery supports both performance and recovery.
Effects beyond muscle
While muscle growth receives the most attention, IGF-1 LR3 affects multiple tissue types throughout the body.
Connective tissue: IGF-1 supports collagen synthesis and can accelerate healing in tendons, ligaments, and other connective tissues. This makes it interesting for recovery from bone and cartilage injuries.
Fat metabolism: IGF-1 LR3 increases lipolysis and enhances glucose metabolism. While not primarily a fat loss compound, these effects support body recomposition when combined with appropriate training and nutrition. Those specifically interested in fat burning peptides may find IGF-1 LR3's secondary metabolic effects beneficial.
Nervous system: IGF-1 has neuroprotective properties and supports cognitive function. The brain contains IGF-1 receptors, and the growth factor plays roles in neural development and maintenance.
Skin and wound healing: Enhanced collagen production and cellular regeneration extend to skin tissue, potentially improving wound healing and tissue repair throughout the body.
IGF-1 LR3 dosage protocols
Dosing IGF-1 LR3 requires balancing effectiveness against potential side effects. Unlike some peptides where more is simply better, IGF-1 LR3 has a relatively narrow therapeutic window. The research literature and clinical reports suggest several dosing approaches depending on experience level and goals.
Beginner protocol
Those new to IGF-1 LR3 should start conservatively to assess individual response and tolerance.
Dosage: 20 to 40 mcg per day
Frequency: Once daily
Administration: Subcutaneous or intramuscular injection
Timing: Post-workout on training days, morning on rest days
Cycle length: 4 to 6 weeks
Time off: Equal to time on (4-6 weeks minimum)
Starting at the lower end of this range allows you to gauge how your body responds before increasing dosage. Some researchers report strong effects even at 20 mcg daily, while others require higher doses for noticeable results.
Intermediate protocol
After establishing tolerance with a beginner protocol, researchers may move to standard dosing.
Dosage: 40 to 60 mcg per day
Frequency: Once daily
Administration: Subcutaneous or intramuscular
Timing: Morning fasted or post-workout
Cycle length: 4 to 6 weeks
Time off: Equal to or longer than time on
This range represents the most common dosing in research protocols. The peptide calculator can help determine injection volumes based on your reconstitution concentration.
Advanced protocol
Experienced researchers sometimes use higher doses, though diminishing returns and increased side effect risk apply.
Dosage: 60 to 100 mcg per day
Frequency: Once daily or split into two doses
Administration: Subcutaneous or intramuscular
Cycle length: 4 to 6 weeks maximum
Time off: Longer than time on
Important: IGF-1 LR3 dosage should not exceed 100 mcg per day according to most research protocols. Higher doses increase side effect risk without proportional benefit increases.
Timing considerations
When you take IGF-1 LR3 affects its efficacy. Two timing strategies dominate the research:
Morning fasted: Administering IGF-1 LR3 in a fasted state maximizes receptor sensitivity. The absence of elevated insulin allows IGF-1 to bind receptors more effectively. This timing works well on non-training days.
Post-workout: Injecting after training capitalizes on elevated blood flow to trained muscles and the anabolic signaling environment that exercise creates. The combination of training-induced mTOR activation plus IGF-1 LR3 may produce synergistic effects.
Both approaches have merit. Some researchers alternate based on training schedule. The key is consistency, taking IGF-1 LR3 at the same time each day helps maintain stable levels given its long half-life.
Cycle length and time off
Using IGF-1 LR3 for too long can lead to reduced effectiveness over time. Receptor desensitization occurs with prolonged exposure, meaning the same dose produces progressively weaker effects. Additionally, extended elevation may increase insulin resistance and other metabolic concerns.
Standard practice limits cycles to 4 to 6 weeks, followed by equal or longer time off. This cycling allows receptors to resensitize and natural hormonal systems to normalize. Both men and women should avoid exceeding 8 weeks of continuous use without breaks.
For guidance on how long peptides take to work, IGF-1 LR3 typically shows effects within the first few weeks, with peak benefits around weeks 3 to 4 of a cycle.
How to reconstitute and store IGF-1 LR3
IGF-1 LR3 typically comes as a lyophilized powder requiring reconstitution before use. The reconstitution process requires more attention than some other peptides because IGF-1 LR3 can be sensitive to certain solvents.
Reconstitution options
Two main reconstitution approaches exist, each with advantages and drawbacks.
Bacteriostatic water: The most common solvent for peptide reconstitution, bacteriostatic water contains benzyl alcohol as a preservative. This allows multiple withdrawals from the same vial. However, some sources indicate that the benzyl alcohol may degrade IGF-1 LR3 structure over time, potentially reducing potency within days to weeks.
Acetic acid solution (0.6%): IGF-1 LR3 remains more stable in dilute acetic acid, maintaining potency for weeks to months when refrigerated. The drawback is that acetic acid can cause tissue irritation at injection sites. Researchers using this method often "back-load" their injection syringe with bacteriostatic water at a 4:1 ratio immediately before injection to dilute the acid and reduce irritation.
For standard use with bacteriostatic water, use the solution within 2 to 4 weeks. For longer storage, acetic acid provides better stability.
Reconstitution procedure
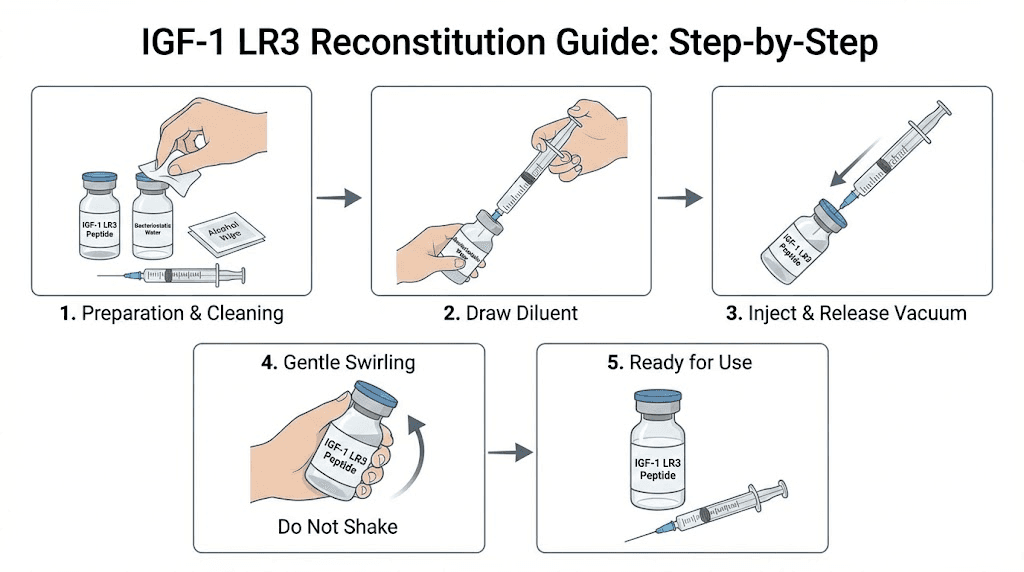
The reconstitution process follows standard peptide reconstitution practices with extra care for this sensitive compound.
Wash hands thoroughly
Clean the tops of both vials with alcohol swabs
Draw your chosen solvent into a sterile syringe
Inject the solvent slowly into the IGF-1 LR3 vial, directing the stream against the glass wall rather than onto the powder
Let the vial sit undisturbed for several minutes, allowing the peptide to dissolve naturally
Gently swirl to mix, never shake vigorously
Confirm the solution is clear with no visible particles
Label with date and concentration
For a 1 mg vial, adding 1 mL of solvent creates a concentration of 1000 mcg/mL. Adding 2 mL creates 500 mcg/mL. Choose a concentration that makes your target dose easy to measure.
Storage requirements
Unreconstituted IGF-1 LR3 can be stored at room temperature short-term but keeps longer under refrigeration. Freezing lyophilized powder is generally safe and extends shelf life significantly.
After reconstitution, storage becomes critical. Keep the vial refrigerated at 36 to 46 degrees Fahrenheit. Do not freeze reconstituted solution. Use within the timeframe appropriate for your solvent choice, typically 2 to 4 weeks for bacteriostatic water or longer for acetic acid.
Protect from light by storing in the original vial or wrapping in foil. For detailed guidance on how long reconstituted peptides last, similar principles apply across most injectable compounds, though IGF-1 LR3 may be more sensitive than average.
Administration and injection technique
IGF-1 LR3 can be administered subcutaneously or intramuscularly. Unlike IGF-1 DES, which benefits from site-specific injection, LR3's long half-life means injection site matters less, the peptide will circulate systemically regardless of where you inject it.
Subcutaneous injection
Subcutaneous administration is the most convenient approach for most researchers. Common injection sites include the lower abdomen lateral to the navel and the outer thigh.
Use an insulin syringe with a short, thin needle, typically 27 to 31 gauge and 5/16 to 1/2 inch length.
Pinch the skin at your chosen site, insert the needle at a 45 to 90 degree angle, inject slowly, and apply light pressure after withdrawal.
Rotate injection sites to prevent irritation or lipodystrophy at any single location. Our peptide injections guide provides detailed technique instructions applicable to IGF-1 LR3 and other subcutaneous peptides.
Intramuscular injection
Some researchers prefer intramuscular administration, particularly when combining with training. While LR3 will distribute systemically regardless, IM injection into a muscle about to be trained might provide slightly enhanced local effects.
IM injection requires longer needles, typically 22 to 25 gauge and 1 to 1.5 inches. Common sites include the deltoid, vastus lateralis, and gluteal muscles. Proper technique requires inserting the needle fully into the muscle before injection.
Practical injection tips
Several practices improve injection experience and consistency:
Allow refrigerated solution to warm slightly before injection to reduce discomfort
Clean injection sites with alcohol and allow to dry completely
Inject slowly rather than rapidly pushing the plunger
Keep a log of injection sites to ensure proper rotation
If using acetic acid reconstitution, dilute with BAC water immediately before injection
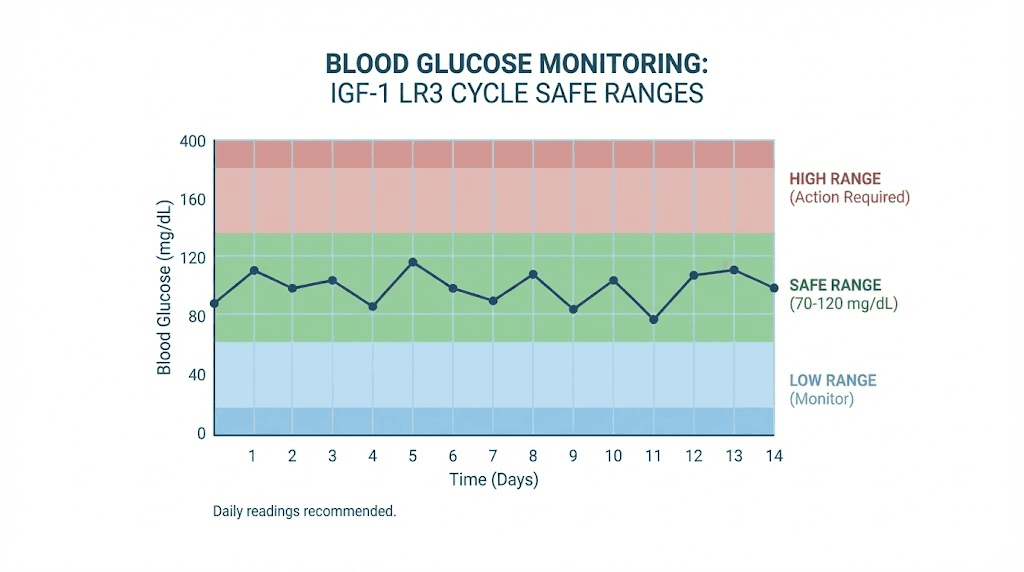
Because IGF-1 can lower blood sugar, having a small carbohydrate source available after injection helps prevent hypoglycemic symptoms. Taking IGF-1 LR3 with some carbohydrates can help keep blood sugar stable.
Stacking IGF-1 LR3 with other peptides
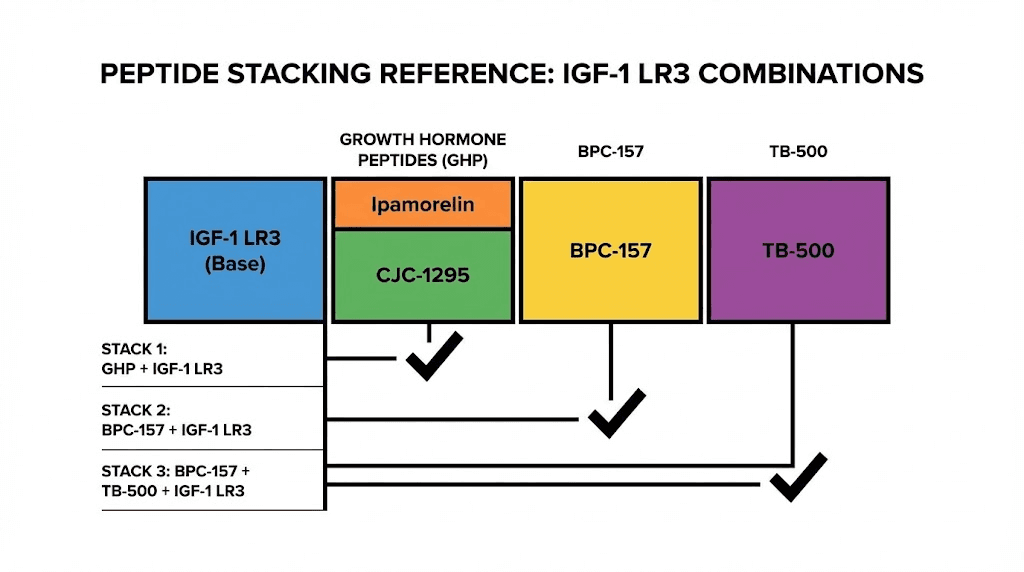
IGF-1 LR3 rarely functions alone in comprehensive research protocols. Strategic stacking with complementary peptides can amplify results while addressing recovery and overall health. The BPC-157 and TB-500 stacking guide covers two of the most common additions.
Recovery stack: BPC-157 and TB-500
The undisputed champions in the recovery peptide category for stacking with IGF-1 LR3 are BPC-157 and TB-500. These peptides complement IGF-1 LR3's anabolic effects by supporting the connective tissue and recovery infrastructure that intense training demands.
BPC-157 promotes angiogenesis, creating new blood vessels that improve nutrient and oxygen delivery to healing tissues. Its primary role involves localized repair at injection sites. For those wondering how to take BPC-157, it can be administered near injury sites for targeted effects or systemically for general recovery support.
TB-500 (Thymosin Beta-4) works systemically to reduce inflammation and promote healing throughout the body. It supports cell migration and differentiation necessary for tissue repair. Unlike BPC-157's localized focus, TB-500 travels throughout the body addressing inflammation wherever it exists.
Sample recovery stack:
IGF-1 LR3: 40-50 mcg daily
BPC-157: 250-500 mcg daily
TB-500: 2-2.5 mg twice weekly
Duration: 4-6 weeks
This combination creates a comprehensive repair environment where IGF-1 LR3 drives muscle protein synthesis while BPC-157 and TB-500 ensure supporting tissues keep pace with rapid muscle development.
Growth hormone stack: CJC-1295 and Ipamorelin
IGF-1 is normally produced in response to growth hormone. Adding growth hormone releasing peptides creates a synergistic environment where both natural and exogenous IGF-1 work together.
CJC-1295 stimulates growth hormone release from the pituitary, while Ipamorelin provides additional GH stimulation through a different mechanism. Combined with IGF-1 LR3, this stack addresses multiple points in the growth hormone axis.
Sample GH stack:
IGF-1 LR3: 40-60 mcg post-workout
CJC-1295 (no DAC): 100 mcg before bed
Ipamorelin: 100-200 mcg before bed
Duration: 4-6 weeks IGF-1 LR3, GH peptides can run longer
The Sermorelin peptide offers another GH-releasing option for those seeking alternatives to CJC-1295.
Performance stack: Wolverine protocol inspiration
The Wolverine stack popularized combining multiple peptides for comprehensive performance enhancement. While that specific stack focuses on different compounds, the philosophy applies to IGF-1 LR3 protocols.
A performance-oriented stack might include:
IGF-1 LR3: 50-80 mcg daily
BPC-157: 250-500 mcg daily
TB-500: 2.5 mg twice weekly
Ipamorelin: 200 mcg pre-bed
This combination addresses muscle growth (IGF-1 LR3), tissue repair (BPC-157, TB-500), and natural GH optimization (Ipamorelin). Such comprehensive stacks require careful monitoring and should only be considered by experienced researchers.
Stacking precautions
Stacking increases both potential benefits and potential risks. Overlapping pathways might amplify side effects or suppress natural hormone function. Insulin sensitivity shifts become more likely when multiple growth-promoting compounds are used simultaneously.
Start conservatively when combining compounds. Don't introduce multiple new peptides at once, as this makes it impossible to determine which compound causes any observed effects or side effects. Build stacks gradually over successive cycles.
IGF-1 LR3 side effects and risks
IGF-1 LR3 carries significant potential side effects that require understanding before use. This isn't a compound to approach casually. The same potent growth-promoting effects that make it attractive also create real risks that demand respect.
Hypoglycemia
The most common and immediately dangerous side effect is hypoglycemia, low blood sugar. IGF-1 has insulin-like effects that increase glucose uptake into cells. When blood sugar drops too low, symptoms can range from uncomfortable to dangerous.
Symptoms of hypoglycemia include anxiety, blurred vision, chills, cold sweats, confusion, dizziness, fast heartbeat, headache, increased hunger, nervousness, shakiness, and unusual tiredness or weakness. Severe hypoglycemia can cause seizures or loss of consciousness.
The risk increases substantially when stacking IGF-1 LR3 with insulin, a practice that should only be considered under strict medical supervision if at all. Even without insulin, researchers should have fast-acting carbohydrates available and monitor for symptoms.
Taking IGF-1 LR3 with some carbohydrates helps prevent blood sugar drops. Don't inject in a completely fasted state if you're sensitive to hypoglycemia.
Cancer considerations
IGF-1 promotes cell growth and inhibits apoptosis, the programmed cell death that normally eliminates abnormal cells. This creates theoretical concerns about cancer risk that require serious consideration.
There is no direct evidence that IGF-1 peptides cause cancer. However, because IGF-1 promotes cell growth, it could theoretically accelerate the progression of existing or dormant tumors. This concern is particularly relevant for hormone-sensitive tissues like breast, prostate, and colon.
Individuals with a history of cancer, active tumors, or strong genetic predisposition to cancer should avoid IGF-1 use entirely. Even for others, this theoretical risk underscores the importance of cycling rather than continuous use.
Insulin resistance
Long-term IGF-1 LR3 use may contribute to insulin resistance. The metabolic effects that promote glucose uptake acutely can, with chronic exposure, lead to cells becoming less responsive to insulin's signals. This is one reason cycling remains important.
Monitoring fasting glucose and considering insulin sensitivity markers during cycles helps identify early signs of metabolic disruption.
Acromegalic effects
Prolonged elevation of IGF-1 can cause changes similar to acromegaly, the condition caused by excess growth hormone in adults. Potential changes include enlarged jaw, hands, feet, and internal organs. While these changes typically require extended exposure at high levels, they represent a real risk of excessive or prolonged use.
One particularly serious concern is acromegalic cardiomyopathy, enlargement and weakening of the heart. If IGF-1 levels remain elevated for extended periods, issues with cardiac rhythm and heart valves may develop. This underscores why cycle limits and adequate time off matter so much.
Other side effects
Additional reported side effects include:
Joint pain and water retention
Muscle and joint aches
Headaches and nausea
Receptor desensitization with prolonged use
Potential suppression of natural GH and IGF-1 production
Who should avoid IGF-1 LR3
Certain groups should not use IGF-1 LR3:
Anyone with active cancer or tumor history
Those with severe insulin resistance or diabetes
Pregnant or nursing women
Anyone under 25 whose growth plates haven't closed
Those with existing hormonal imbalances
IGF-1 LR3 is not FDA-approved for general medical use and remains primarily a research compound. Understanding peptide legality in your jurisdiction matters before beginning any research.
Expected results and realistic expectations
Setting realistic expectations helps avoid disappointment and dangerous dose escalation. IGF-1 LR3 is potent, but it's not magic. Results depend heavily on training, nutrition, and individual response.
What to expect
Weeks 1-2: Most researchers notice improved recovery and possibly enhanced "pump" during training. Strength may begin increasing. These early effects help confirm the compound is active but don't represent full results.
Weeks 3-4: More noticeable effects typically emerge. Improved muscle fullness, continued strength gains, and potentially visible body composition changes. This is often when IGF-1 LR3 cycles show their peak effects.
Weeks 5-6: Continued progress, though rate of improvement may slow as receptors begin to desensitize. This is typically when cycles end.
Documented results from research protocols suggest modest but meaningful improvements. Don't expect steroid-like transformations. IGF-1 LR3 works more subtly, optimizing natural processes rather than overriding them completely.
For context on what's achievable, peptides before and after results vary widely based on individual factors, training quality, and nutritional support.
Factors affecting results
Training: IGF-1 LR3 enhances adaptation to training stimulus. Without adequate training, results will disappoint. The compound amplifies what you're already doing rather than replacing the need for hard work.
Nutrition: Protein intake must be adequate to support increased protein synthesis. Caloric intake should match goals, whether building muscle or recomposition. Carbohydrate timing around IGF-1 administration helps manage blood sugar.
Sleep and recovery: Much of muscle building occurs during rest. Skimping on sleep undermines IGF-1 LR3's potential effects.
Individual response: Some researchers respond dramatically to IGF-1 peptides while others notice minimal effects. Genetic factors in receptor density and sensitivity play significant roles.
Comparing to other options
IGF-1 LR3 occupies a specific niche in the performance peptides landscape. Compared to growth hormone releasing peptides, it works downstream in the growth pathway, directly stimulating tissues rather than triggering natural GH release. Compared to steroids, effects are more modest but with potentially fewer side effects and easier recovery.
The peptides versus steroids comparison explores these differences in detail. Understanding where IGF-1 LR3 fits helps set appropriate expectations.
Monitoring and blood work
Responsible IGF-1 LR3 use includes monitoring to catch potential issues early and optimize protocols based on individual response.
Pre-cycle testing
Before starting IGF-1 LR3, establish baseline values for:
Fasting glucose and insulin
HbA1c (long-term blood sugar marker)
IGF-1 levels
Complete metabolic panel
Lipid panel
These baselines allow comparison during and after cycles to identify any negative trends.
During cycle monitoring
Track fasting blood glucose regularly, even daily if you have a home glucose monitor. This provides early warning of hypoglycemia patterns or developing insulin resistance.
Watch for symptoms of hypoglycemia, especially in the hours following injection. Keep a log of any unusual symptoms including joint pain, headaches, or changes in how you feel.
Mid-cycle blood work at around week 3-4 can identify any concerning trends before they become serious issues.
Post-cycle assessment
After completing a cycle, repeat baseline blood work to ensure metabolic markers have normalized. Give it 2-4 weeks after your last injection before testing, allowing the long half-life of LR3 to clear fully.
If any markers show negative changes, extend time off before considering another cycle. Persistent metabolic disruption is a signal to reconsider whether IGF-1 LR3 is appropriate for your situation.
Legal status and obtaining IGF-1 LR3
Understanding the regulatory framework around IGF-1 LR3 matters for anyone considering its use. The compound occupies a complex legal space that varies by jurisdiction.
Regulatory status
IGF-1 LR3 is not FDA-approved for any medical use in humans. It's classified as a research chemical, meaning it can be legally purchased for research purposes but not for human consumption in most jurisdictions.
The World Anti-Doping Agency (WADA) bans IGF-1 variants in competitive sports. Athletes subject to drug testing should be aware that IGF-1 LR3 is a prohibited substance.
For current information on peptide regulations, rules continue evolving as regulatory agencies address these compounds.
Quality considerations
Because IGF-1 LR3 isn't regulated as a pharmaceutical, product quality varies dramatically between sources. Key considerations when evaluating sources include:
Third-party testing for identity and purity
Proper cold-chain shipping to maintain stability
Clear labeling of contents and concentrations
Reputation within research communities
The peptide testing labs guide covers how to verify product quality through independent analysis. Given IGF-1 LR3's sensitivity and the significant investment involved, verification provides important assurance.
Finding clinical guidance
Those seeking medically supervised peptide protocols should consult with qualified practitioners. The peptide therapy near me guide and location-specific resources for cities like Houston, Austin, Phoenix, and Atlanta can help locate knowledgeable providers.
Working with medical oversight provides access to prescription-grade compounds, proper monitoring, and professional guidance on dosing and cycling.
Frequently asked questions
Is IGF-1 LR3 legal to purchase?
IGF-1 LR3 is legal to purchase as a research chemical in most jurisdictions, including the United States.
However, it is not approved for human use by the FDA and is banned in competitive sports by WADA. Understanding peptide legality in your specific location is important before purchasing.
How long does it take IGF-1 LR3 to work?
Most researchers notice initial effects like improved recovery and muscle pumps within the first 1-2 weeks. More significant results typically emerge around weeks 3-4. Full effects develop over a complete 4-6 week cycle. Individual response varies considerably, with some noticing effects earlier than others.
Can IGF-1 LR3 be stacked with steroids?
Yes, IGF-1 LR3 is sometimes combined with anabolic steroids in advanced protocols. This combination can produce synergistic effects but also increases complexity and risk. Such stacks should only be considered by experienced researchers with thorough understanding of both compound classes.
The peptides versus steroids comparison provides context on how these compound classes interact.
Does IGF-1 LR3 require injection into specific muscles?
No, unlike IGF-1 DES which benefits from site-specific injection, IGF-1 LR3's long half-life means it circulates systemically regardless of injection site. Subcutaneous injection in the abdomen or thigh works well. The peptide will distribute throughout the body and affect all tissues with IGF-1 receptors.
How should I store IGF-1 LR3?
Unreconstituted powder can be stored refrigerated or frozen for extended periods. After reconstitution, keep refrigerated at 36-46°F and use within 2-4 weeks for bacteriostatic water reconstitution, or longer for acetic acid. Never freeze reconstituted solution. Protect from light. Check peptide expiration guidance for storage best practices.
What's the difference between IGF-1 LR3 and IGF-1 DES?
IGF-1 LR3 has a 20-30 hour half-life and works systemically throughout the body, making it ideal for overall muscle growth with once-daily dosing. IGF-1 DES has a 20-30 minute half-life but is about 10x more potent, making it best for localized, site-specific applications where it's injected directly into target muscles before training.
Can women use IGF-1 LR3?
Yes, women can use IGF-1 LR3 at similar or slightly lower doses than men. The compound affects both sexes similarly since IGF-1 receptor distribution doesn't differ significantly between men and women. Starting at the lower end of dosing ranges (20-30 mcg) and assessing response before increasing is advisable.
Does IGF-1 LR3 cause hair loss?
IGF-1 LR3 is not associated with hair loss. In fact, IGF-1 may support hair follicle health in some cases, though this isn't a primary use. Unlike androgens that can accelerate male pattern baldness, IGF-1's growth-promoting effects don't specifically target hair follicles negatively.
For researchers committed to understanding growth factor peptides thoroughly, SeekPeptides provides comprehensive protocols, dosing guidance, and community support.
Members access detailed information on IGF-1 variants and other injectable peptides, helping navigate the complexities of peptide research safely and effectively.