Jan 21, 2026

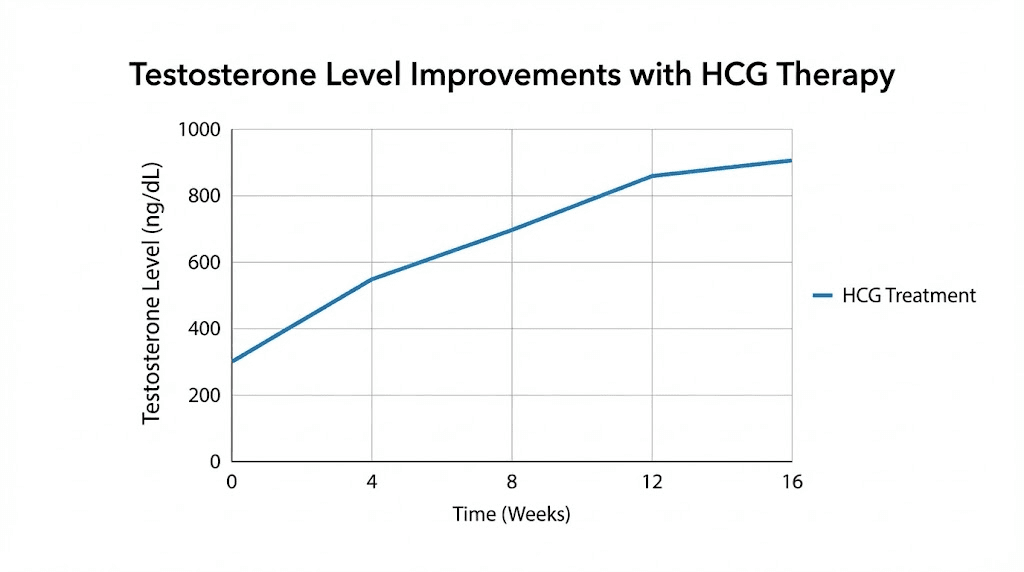
Of the men who use HCG alongside testosterone therapy, studies show a 223% increase in testosterone levels.
That number comes from randomized clinical research. Not marketing claims. Not bro science. Actual peer-reviewed data.
But here's what makes HCG uniquely valuable. Unlike exogenous testosterone that shuts down your natural production, HCG works with your body's existing machinery. It mimics luteinizing hormone. It tells your testes to keep working. And it does all of this while potentially preserving your natural testosterone production and fertility.
The challenge? Most information about HCG online mixes medical uses with weight loss scams that the FDA explicitly warns against. Finding accurate, actionable guidance requires sifting through contradictory advice, outdated protocols, and outright misinformation. This guide cuts through that noise.
Whether you're considering HCG for testosterone support, fertility preservation during TRT, post-cycle therapy, or as a standalone treatment, the following pages cover everything you need to make informed decisions. We'll examine mechanisms, dosing protocols, reconstitution methods, side effect management, and when HCG makes sense versus when alternatives might serve you better. SeekPeptides members often ask about HCG because it addresses one of the most common concerns in hormone optimization, maintaining testicular function while supporting healthy testosterone levels.
What is HCG and why it matters for men
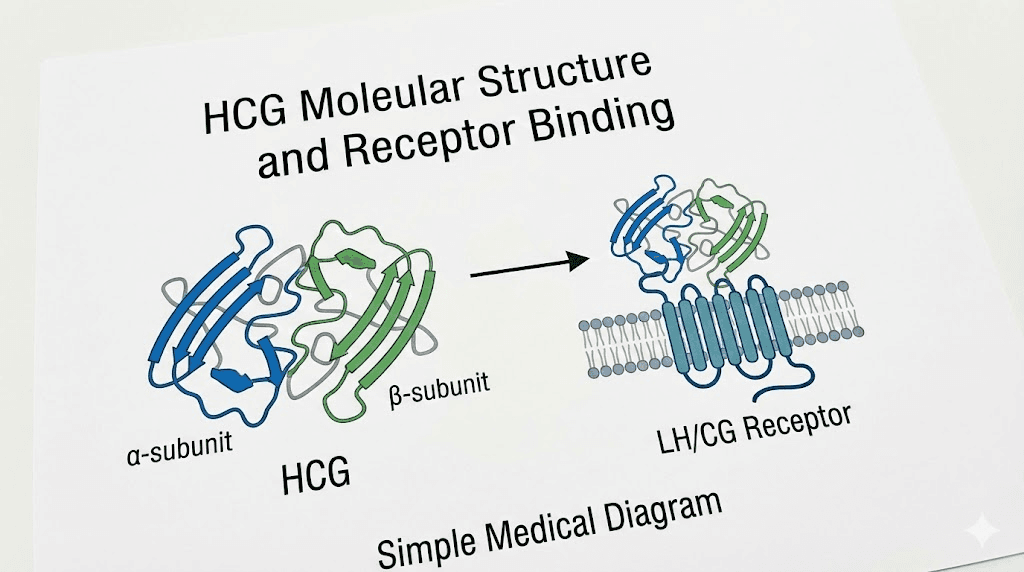
Human chorionic gonadotropin is a glycoprotein hormone composed of 237 amino acids with a molecular mass of 36.7 kilodaltons. The body naturally produces HCG during pregnancy, where it maintains the corpus luteum and supports early fetal development. But this pregnancy hormone has found a second life in men's health, specifically for testosterone support and fertility preservation.
The hormone consists of two subunits.
An alpha subunit identical to those found in luteinizing hormone, follicle-stimulating hormone, and thyroid-stimulating hormone. And a beta subunit that gives HCG its unique biological activity. This structural similarity to LH is exactly why HCG works in men. Your Leydig cells can't tell the difference between natural LH and administered HCG.
For researchers exploring peptides for men, understanding HCG's classification matters. Technically, HCG is a protein hormone rather than a peptide in the strict sense, since it exceeds the typical peptide size threshold. However, it's commonly discussed alongside injectable peptides because of its similar administration methods and its role in hormone optimization protocols.
The FDA has approved HCG for specific medical uses in men. These include treating hypogonadism, addressing male infertility, and managing prepubertal cryptorchidism. Currently, both urinary-derived and recombinant HCG preparations are commercially available, giving researchers and clinicians multiple sourcing options depending on their specific needs and local peptide regulations.
Why HCG has become essential in men's hormone optimization
Testosterone replacement therapy changes lives. It restores energy, improves body composition, enhances mood, and revitalizes libido. But TRT comes with a fundamental trade-off that many men don't fully understand until they're deep into treatment. When you add exogenous testosterone, your body responds by reducing its own production.
This feedback mechanism affects more than just testosterone output. Your pituitary gland decreases luteinizing hormone secretion. Your testes receive less stimulation. They shrink. Sometimes significantly. And if fertility matters to you, the news gets worse. Sperm production can decline dramatically or cease entirely.
HCG addresses these concerns directly. By mimicking LH, it keeps the testes active even when the pituitary has reduced its natural LH output. This maintains testicular volume, preserves intratesticular testosterone levels necessary for sperm production, and provides a backup testosterone source that works synergistically with TRT. For men who want the benefits of peptides for muscle growth and hormone optimization without sacrificing their fertility, HCG often becomes an essential protocol component.
How HCG works in the male body
Understanding HCG's mechanism requires a brief tour of the hypothalamic-pituitary-gonadal axis. Your hypothalamus releases gonadotropin-releasing hormone in pulses. This stimulates the pituitary to secrete LH and FSH. LH then travels to your testes and binds to receptors on Leydig cells, triggering testosterone synthesis. FSH supports Sertoli cells, which are essential for sperm production.
HCG enters this system as an LH analog. It binds to the same LHCG receptors on Leydig cells, activating the same cellular cascades that natural LH would trigger. The result? Testosterone production continues even when your pituitary has stopped sending LH signals.
The intratesticular testosterone this produces serves a purpose beyond what shows up in blood tests. Sertoli cells need extremely high local testosterone concentrations to support spermatogenesis. Blood testosterone levels of 500 ng/dL might require intratesticular levels 50 to 100 times higher. Only local production within the testes can achieve these concentrations. This is why injecting testosterone alone doesn't preserve fertility, but adding HCG often can.
Research from Baylor College of Medicine demonstrated this effect clearly. Men on testosterone therapy who received 500 IU of HCG every other day maintained intratesticular testosterone levels 26% above baseline. Those receiving only 250 IU saw levels drop 7% below baseline. The difference in dosing determined whether testicular function was preserved or compromised.
HCG's effects on testosterone and sperm production
Clinical data paints a consistent picture of HCG's effectiveness. In hypogonadic men with severe oligozoospermia, HCG therapy improved sperm concentration from 3.03 million per milliliter to 6.54 million per milliliter after three months. That's more than doubling the count in men who had almost no viable sperm to begin with.
The timeline matters too. Most men see initial testosterone increases within the first few weeks. Spermatogenesis takes longer. Studies show occasional sperm appearing around month three, with more significant improvements by month four to six. Some men achieve normal semen parameters, while others show substantial improvement without reaching normal ranges.
For men recovering from testosterone-induced azoospermia, the picture is encouraging. A 2024 study found that total sperm count increased from 18 million to 146.9 million after HCG treatment. The number of men with normal total motile sperm count jumped from 5% to 58%. These aren't small improvements. They're potentially life-changing for men who want to father children.
The HMG peptide provides similar benefits through a different mechanism, stimulating both LH and FSH pathways. Some protocols combine HCG with HMG or FSH for enhanced spermatogenic effects, particularly in cases where HCG monotherapy hasn't restored adequate sperm parameters.
Medical uses of HCG in men
The FDA has approved HCG for several male health conditions, but its off-label uses have expanded far beyond original indications. Understanding both approved and research applications helps frame realistic expectations.
Treating hypogonadism
Hypogonadism, where the body produces insufficient testosterone, affects millions of men. Symptoms include fatigue, reduced libido, depression, decreased muscle mass, and cognitive fog. Traditional treatment involves testosterone replacement, but HCG offers an alternative pathway that some men prefer.
HCG monotherapy has shown promise for men with symptomatic testosterone deficiency. Multi-institutional research found mean testosterone improved by 49.9% in men starting with levels around 362 ng/dL. Half of patients reported significant symptom improvement. Another study of 31 patients showed 86% improvement in erectile dysfunction and 80% improvement in libido with HCG alone.
The appeal of HCG monotherapy lies in what it preserves. Unlike exogenous testosterone, HCG maintains testicular volume, preserves fertility potential, and avoids complete shutdown of the HPG axis. For younger men who might want children in the future, or for those who prefer a more natural approach to hormone optimization, HCG monotherapy presents an option worth discussing with healthcare providers. SeekPeptides provides detailed protocols for various hormone support approaches, helping members understand their options.
Supporting fertility during testosterone therapy
The most common use of HCG in men's health involves concurrent administration with testosterone replacement therapy.
This combination aims to provide the benefits of TRT while mitigating its most significant drawback, fertility suppression.
Research suggests this approach works. The Baylor study mentioned earlier showed that men receiving 500 IU every other day maintained normal sperm parameters while on testosterone therapy. Nine of 26 participants achieved pregnancy with their partners during the study period. For men who need TRT but aren't ready to close the door on fatherhood, this combination offers a middle path.
The protocol typically involves starting HCG when beginning testosterone therapy, though some practitioners add it later if testicular atrophy becomes noticeable. Timing matters less than consistency. Once the testes have experienced significant atrophy, recovery becomes more difficult, though rarely impossible.
Post-cycle therapy applications
Men who use anabolic steroids for athletic or physique purposes face a particular challenge when discontinuing these compounds. The HPG axis, suppressed during steroid use, needs time to recover. Without intervention, this recovery can take months, during which testosterone levels remain dangerously low.
HCG serves a specific role in post-cycle therapy. By stimulating the testes directly, it helps maintain their function during the transition period while the pituitary slowly resumes normal LH production. Common PCT protocols use 1000 to 2000 IU every other day for one to two weeks before ending testosterone, continuing for another one to two weeks after.
The peptides versus SARMs comparison often includes discussion of PCT requirements. While SARMs may suppress testosterone less severely than traditional steroids, many users still benefit from structured recovery protocols that include HCG.
Treating cryptorchidism
In prepubertal boys, HCG can help descend undescended testes, addressing cryptorchidism without surgical intervention. This medical application demonstrates HCG's ability to stimulate testicular growth and development, effects that carry over into its use in adult men.
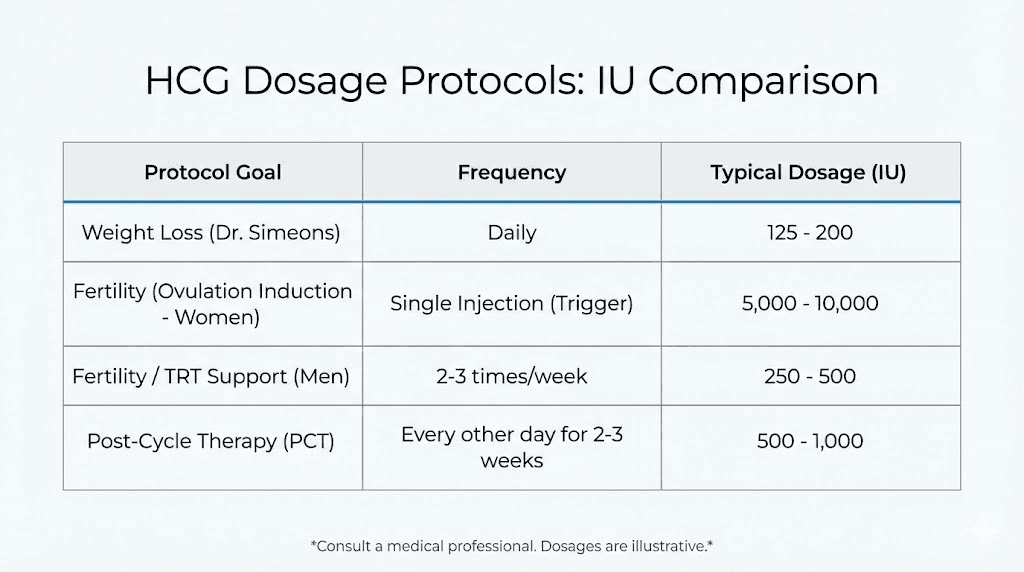
HCG dosage protocols for different goals
Dosing HCG correctly requires matching the protocol to your specific goals. A fertility-focused approach differs significantly from a testicular maintenance protocol. Getting this wrong means either wasting resources on insufficient doses or risking side effects from excessive administration.
HCG dosing for testosterone support with TRT
When using HCG alongside testosterone therapy primarily for testicular maintenance rather than active fertility preservation, lower doses often suffice. Most clinical protocols recommend 500 to 1000 IU administered one to three times weekly. This provides enough stimulation to maintain testicular volume and function without significantly elevating estrogen or causing other issues.
The lower end of this range, around 500 IU twice weekly, works well for men whose primary concern is preventing testicular atrophy. They're not actively trying to conceive but want to maintain the option. This dosing typically keeps intratesticular testosterone levels adequate for general testicular health without maximizing sperm production.
For reference, the peptide calculator can help with general dosing calculations, though HCG dosing specifically requires understanding the IU (international unit) system rather than milligram measurements used for most peptide dosages.
HCG dosing for fertility preservation
Men actively trying to preserve or restore fertility while on TRT need higher, more consistent dosing. The research-backed protocol uses 500 IU administered subcutaneously or intramuscularly every other day, equivalent to approximately three times weekly.
This dosing proved effective in maintaining normal sperm parameters in the Baylor study. Importantly, doses below 500 IU every other day showed inferior results. Men receiving 250 IU at the same frequency saw intratesticular testosterone drop below baseline, potentially compromising spermatogenesis.
For men who desire pregnancy within six months and have been on TRT, some practitioners recommend discontinuing testosterone entirely and increasing HCG to 3000 IU every other day. This aggressive approach maximizes testicular stimulation while removing the suppressive effects of exogenous testosterone. Combined with clomiphene citrate in some protocols, this strategy aims for the fastest possible restoration of fertility.
HCG dosing for post-cycle therapy
PCT protocols typically use higher doses than maintenance protocols but for shorter durations. A common approach involves 1000 to 2000 IU every other day during the transition period. Some practitioners recommend starting HCG one to two weeks before the last testosterone injection, then continuing for two to four weeks after.
The goal differs from ongoing TRT support. PCT aims to maintain testicular function during a specific recovery window while the HPG axis restores natural LH production. Once natural production resumes, HCG is discontinued to avoid potential desensitization issues.
Higher doses, up to 3000 IU three times weekly, may be used for men recovering from particularly suppressive cycles. However, exceeding 5000 IU weekly increases risks without proportional benefits for most users.
HCG monotherapy dosing
Men using HCG as their sole testosterone support need dosing adequate to stimulate meaningful testosterone production. Research on HCG monotherapy shows effectiveness at various doses, but most protocols settle around 1500 to 3000 IU weekly, divided into multiple injections.
A typical monotherapy protocol might involve 500 IU three times weekly or 750 IU every other day. These doses produce testosterone increases of 40 to 80% above baseline in most men, often pushing levels into the normal or high-normal range.
The key advantage of monotherapy is preserved HPG axis function. Unlike TRT, which completely shuts down natural LH production, HCG monotherapy only partially suppresses the axis. Some natural pulsatile hormone release continues. For men with mildly low testosterone who want improvement without full replacement therapy, this approach offers a meaningful alternative.
How to reconstitute and store HCG
HCG typically arrives as a lyophilized powder that requires reconstitution before use. This process is straightforward but requires attention to sterile technique to avoid contamination. If you're familiar with reconstituting other peptides with bacteriostatic water, the process will feel familiar.
Supplies needed for reconstitution
Gather your materials before starting.
You'll need bacteriostatic water, the HCG vial containing lyophilized powder, alcohol swabs for sterilization, a sterile syringe for mixing, and appropriate needles. Typical setups use a 3 mL syringe with a 22-gauge needle for reconstitution and a 27-gauge or smaller needle for injection.
Using bacteriostatic water rather than sterile water matters significantly for shelf life. Bacteriostatic water contains benzyl alcohol, an antimicrobial agent that prevents bacterial growth in the reconstituted solution. This allows for multiple withdrawals from the same vial over several weeks without contamination risk.
Step-by-step reconstitution process
Start by washing your hands thoroughly for at least 20 seconds. Clean the tops of both vials, the bacteriostatic water and the HCG powder, with alcohol swabs. Allow them to dry completely before proceeding.
Draw the appropriate amount of bacteriostatic water into your syringe. For a 5000 IU vial, 5 mL of water creates a concentration of 1000 IU per milliliter. For a 10,000 IU vial, 10 mL creates the same concentration. Some users prefer different concentrations based on their injection volume preferences.
Insert the needle into the HCG vial at an angle, directing the stream of bacteriostatic water down the inside wall of the glass. This gentle approach protects the delicate hormone structure. Never shoot the liquid directly onto the powder.
After adding the water, swirl the vial gently until the powder dissolves completely. Do not shake vigorously. The solution should become clear without visible particles. Once reconstituted, label the vial with the date and concentration.
The peptide reconstitution calculator can help determine appropriate water volumes for your specific vial size and desired concentration, though remember HCG is measured in IU rather than milligrams.
Storage requirements
Before reconstitution, lyophilized HCG can be stored at room temperature, though refrigeration extends its shelf life. Once you add bacteriostatic water, refrigeration becomes mandatory. Store reconstituted HCG at 36 to 46 degrees Fahrenheit (2 to 8 degrees Celsius).
Properly stored reconstituted HCG remains potent for 60 to 90 days. Some manufacturers recommend shorter durations. Check your specific product's documentation for guidance. Protect the solution from light by keeping it in the original vial or wrapping with foil.
If you accidentally leave reconstituted HCG at room temperature for several hours, it's likely still usable. However, avoid extended periods above refrigerator temperature. More than 72 hours at room temperature warrants discarding the solution. For general guidance on how long reconstituted peptides last in the fridge, similar principles apply across most injectable compounds.
Administration methods and injection technique
HCG can be administered subcutaneously or intramuscularly. Both routes are effective, though subcutaneous injection has become more popular due to ease and comfort. The choice often comes down to personal preference and practitioner recommendation.
Subcutaneous injection
Subcutaneous administration involves injecting into the fatty tissue just beneath the skin. Common sites include the lower abdomen, lateral to the navel, and the outer thigh. Use an insulin syringe with a short, thin needle, typically 27 to 31 gauge and 5/16 to 1/2 inch in length.
Pinch a fold of skin at your chosen injection site. Insert the needle at a 45 to 90 degree angle, depending on your body composition and needle length. Inject slowly, remove the needle, and apply light pressure with a cotton ball or gauze. Rotate injection sites to prevent localized tissue issues.
For those new to self-injection, our peptide injections guide provides detailed visual instructions applicable to HCG and other injectable compounds.
Intramuscular injection
Intramuscular injection delivers HCG into muscle tissue, typically the deltoid (upper arm) or the vastus lateralis (outer thigh). This method uses slightly longer needles, usually 22 to 25 gauge and 1 to 1.5 inches, depending on muscle mass and body composition.
Intramuscular injection may provide slightly faster absorption, though clinical outcomes appear similar between routes for HCG. Some practitioners prefer IM for higher volume injections, reserving subcutaneous for smaller doses.
Injection frequency considerations
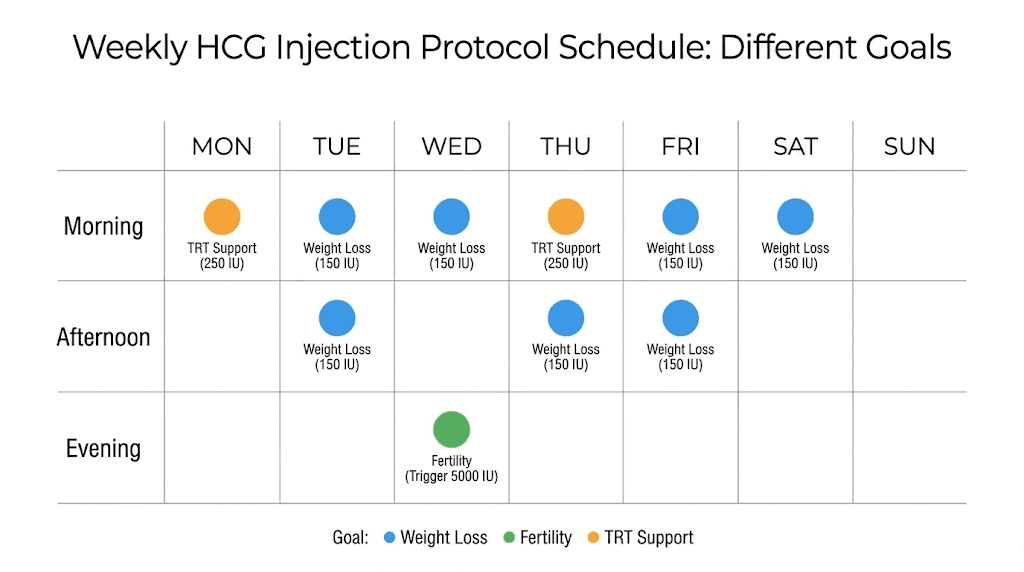
Unlike testosterone with its various ester formulations affecting release timing, HCG has a relatively short half-life requiring multiple weekly administrations. Most protocols involve injecting every other day or three times weekly.
Spreading doses across the week mimics the body's natural pulsatile hormone release better than infrequent large injections. This approach may reduce estrogen spikes and provide more stable testicular stimulation. For men also using testosterone, coordinating injection schedules can simplify the routine.
HCG side effects and risk management
Like any hormone manipulation, HCG use carries potential side effects. Understanding these risks allows for proactive management rather than reactive problem-solving. Most men tolerate HCG well, but awareness prepares you for what might occur.
Estrogen-related effects
HCG stimulates testosterone production in the testes. Some of that testosterone converts to estradiol through aromatase activity. Unlike exogenous testosterone, where aromatization occurs throughout the body, HCG-induced aromatization happens locally in the testes, which contain significant aromatase enzyme.
This can lead to elevated estrogen despite testosterone levels that wouldn't typically cause such elevation with TRT alone. Symptoms of high estrogen include water retention, mood changes, decreased libido, and in some cases, breast tissue sensitivity or gynecomastia.
Management typically involves estrogen monitoring through blood tests and, when necessary, aromatase inhibitors or selective estrogen receptor modulators. Some men find that adjusting HCG dose downward resolves estrogen issues without additional medications.
Gynecomastia risk
Breast tissue development represents one of the more concerning potential side effects, particularly because gynecomastia can become permanent if excessive tissue growth occurs. The risk appears higher in men combining TRT with HCG compared to either alone, likely due to cumulative estrogen effects.
Bloodwork helps identify susceptibility. Men with naturally high aromatase activity or those whose estrogen rises disproportionately to testosterone increases face greater risk. Preventive use of SERMs like tamoxifen can block estrogen receptors in breast tissue without affecting estrogen elsewhere in the body.
If you notice breast tenderness, nipple sensitivity, or tissue changes, address the issue promptly. Discontinuing or reducing HCG often resolves early symptoms. Established gynecomastia may require surgical correction.
Leydig cell desensitization
One theoretical concern with HCG involves potential desensitization of Leydig cells to LH stimulation. The argument suggests that prolonged high-dose HCG exposure might downregulate LH receptors, reducing future testosterone response.
Clinical evidence for this concern remains limited at therapeutic doses. Most studies showing desensitization effects used doses far exceeding clinical protocols. However, the concern supports keeping HCG doses at the minimum effective level rather than maximizing intake.
Doses exceeding 5000 IU weekly rarely provide additional benefits and may increase risks. For most applications, 1500 to 3000 IU weekly achieves therapeutic goals while minimizing potential long-term receptor impacts.
Other potential side effects
Additional side effects, while less common, include headaches, fatigue, mood changes, injection site reactions, and acne. These typically respond to dose adjustment or resolve spontaneously as the body adapts to HCG administration.
Rare but serious complications include blood clots and allergic reactions.
While the overall safety profile of HCG is favorable based on decades of medical use, any unusual symptoms warrant medical evaluation.
A study of 175 men taking HCG injections found no significant adverse side effects, supporting its general safety profile when used appropriately. However, individual responses vary, and monitoring remains important.
HCG compared to alternatives
HCG isn't the only option for men seeking to maintain testicular function or boost testosterone naturally. Understanding how it compares to alternatives helps determine the best approach for individual situations.
HCG versus clomiphene citrate
Clomiphene, commonly known by its brand name Clomid, works differently than HCG. Instead of directly stimulating the testes, clomiphene blocks estrogen receptors in the hypothalamus and pituitary. This tricks the brain into perceiving low estrogen, triggering increased LH and FSH release.
A randomized study compared these approaches directly. Testosterone levels increased by 223% with no significant difference between groups. Both treatments effectively restored testosterone. However, clomiphene also raises estrogen due to its indirect mechanism, potentially causing similar estrogenic side effects as HCG.
Clomiphene offers oral administration, eliminating injection requirements. For men who strongly prefer pills over needles, this convenience factor weighs heavily. The changing regulatory landscape has also affected HCG availability in some regions, making alternatives more attractive.
HCG versus enclomiphene
Enclomiphene represents the active trans-isomer of clomiphene citrate. Unlike clomiphene, which contains both active enclomiphene and the less desirable zuclomiphene isomer, pure enclomiphene provides benefits without some downsides.
Notably, enclomiphene doesn't raise estrogen like clomiphene or HCG. This makes it attractive for men concerned about estrogenic side effects. Studies show similar testosterone increases with potentially fewer mood-related side effects.
Enclomiphene also comes in oral form. The main drawback involves regulatory status. While increasingly available through clinics and compounding pharmacies, enclomiphene lacks FDA approval, which can affect insurance coverage and availability.
For detailed comparison with similar compounds, the Testagen peptide guide covers various testosterone-supporting compounds.
When to choose HCG over alternatives
Several situations favor HCG specifically. If you're using testosterone replacement therapy and want to maintain testicular function, HCG provides direct testicular stimulation that oral medications cannot match while on TRT. The exogenous testosterone suppresses your pituitary regardless of what other oral medications you take.
For men recovering from anabolic steroid use, HCG offers rapid testicular stimulation during the transition period before oral SERMs become effective. The combination of HCG followed by clomiphene or enclomiphene often works better than either alone.
If fertility is the primary concern and you're not on TRT, either HCG or clomiphene can work, with the choice often coming down to personal preference regarding injection versus oral administration.
HCG protocols for specific situations
Different goals require different approaches. The following protocols represent common clinical strategies, though individual optimization should involve healthcare provider guidance.
Protocol for men starting TRT
Beginning HCG when starting testosterone therapy prevents testicular atrophy before it occurs. This proactive approach is easier than reversing established shrinkage.
Goal: Maintain testicular volume and function during TRT
Approach:
HCG 500 IU subcutaneously every other day (3x weekly)
Begin same time as testosterone therapy
Continue for duration of TRT
Monitoring:
Baseline testosterone, estradiol, LH, FSH
Recheck at 6 weeks, then quarterly
Adjust based on estrogen response
Expected results:
Maintained testicular size
Preserved fertility potential
Possible slight testosterone boost above TRT alone
Protocol for fertility restoration on TRT
Men on TRT who want to conceive face a decision. Discontinue testosterone entirely or attempt conception while maintaining therapy. HCG makes the latter option viable for many.
Goal: Maximize sperm production while on testosterone therapy
Approach:
HCG 500 IU subcutaneously every other day
Consider adding FSH or HMG if response insufficient after 3 months
Semen analysis at baseline, 3 months, and 6 months
Timeline:
Initial testosterone response: 2-4 weeks
Sperm appearance: 3-4 months
Significant count improvement: 4-6 months
If conception remains the urgent priority, discontinuing TRT while increasing HCG to 3000 IU every other day accelerates recovery. Some protocols add clomiphene or HMG for additional FSH support.
Protocol for post-cycle therapy
Recovery from anabolic steroid cycles requires supporting the HPG axis while it restores natural function. HCG bridges the gap between cycle end and natural LH production resumption.
Goal: Maintain testicular function and support recovery
Approach:
Begin HCG 1500-2000 IU every other day during final 2 weeks of cycle
Continue for 2-3 weeks after last steroid dose
Transition to SERM (clomiphene 50mg daily for 2 weeks, then 25mg for 2 weeks)
Discontinue HCG when starting SERM
Monitoring:
Blood work at 4 weeks post-cycle
Verify testosterone recovery before discontinuing SERM
For additional context on recovery protocols, our guide on peptides versus steroids discusses differences in recovery requirements.
Protocol for HCG monotherapy
Men preferring to avoid exogenous testosterone can use HCG alone for modest testosterone increases while preserving HPG axis function and fertility.
Goal: Increase testosterone naturally without TRT
Approach:
HCG 1500-3000 IU weekly, divided into 3 injections
Example: 750 IU Monday, Wednesday, Friday
Adjust based on response and symptoms
Expected results:
Testosterone increase of 40-80% above baseline
Symptom improvement in 50-80% of men
Maintained fertility
Limitations:
Ceiling effect, can't achieve supraphysiological levels
May not provide adequate testosterone for all men
Requires ongoing injections
Who should and shouldn't use HCG
HCG offers significant benefits for appropriate candidates but isn't suitable for everyone. Understanding selection criteria helps determine whether HCG deserves consideration in your protocol.
Ideal candidates for HCG
Several groups derive particular benefit from HCG therapy:
Men on TRT who want fertility preservation: If you're taking testosterone replacement therapy but might want children someday, HCG provides insurance against complete fertility loss. Even if fatherhood isn't an immediate goal, maintaining the option has value.
Men experiencing testicular atrophy on TRT: Shrinking testes affect more than appearance. Some men report decreased well-being, reduced ejaculate volume, and psychological discomfort. HCG can reverse this atrophy in most cases.
Men with mild hypogonadism preferring natural approaches: If your testosterone is low but not severely depleted, HCG monotherapy might raise levels adequately without committing to lifelong TRT. This appeals to men who want to preserve natural function while addressing symptoms.
Men recovering from steroid cycles: Anyone who has used anabolic steroids and wants to recover natural testosterone production benefits from HCG during the transition period. It maintains testicular function while the HPG axis restores signaling.
Men with documented LH deficiency: Secondary hypogonadism, where low testosterone results from inadequate pituitary signaling rather than testicular failure, responds particularly well to HCG. The testes can produce testosterone; they just need the signal.
Who should avoid HCG
Men with prostate concerns: While HCG itself doesn't directly affect the prostate, the testosterone it stimulates can. Men with active prostate issues should consult urologists before beginning any testosterone-enhancing protocol.
Men with hormone-sensitive cancers: Certain testicular cancers and some other malignancies can be stimulated by gonadotropins. HCG is actually used as a tumor marker in some cancers because certain tumors produce it.
Men primarily using HCG for weight loss: The FDA explicitly warns that HCG has not been proven effective for weight loss. Products marketed for this purpose often combine HCG with severely restrictive diets. Any weight loss results from the diet, not the HCG. The peptides for weight loss guide covers compounds with actual evidence for metabolic support.
Men who can't commit to regular injections: HCG requires multiple weekly injections. Unlike long-acting testosterone formulations that might be administered biweekly or less, HCG works best with every-other-day or thrice-weekly dosing. Men who can't or won't maintain this schedule should consider oral alternatives.
Combining HCG with other compounds
HCG rarely functions in isolation. Understanding how it interacts with other compounds helps optimize protocols and avoid conflicts.
HCG with testosterone
The most common combination pairs HCG with testosterone replacement therapy. This synergy allows men to receive reliable testosterone levels from exogenous sources while HCG maintains testicular function that TRT would otherwise suppress.
Timing doesn't need to be precise. Some men inject testosterone and HCG on the same days; others stagger them throughout the week. The key is maintaining consistent HCG dosing regardless of testosterone schedule.
This combination may require additional estrogen management compared to TRT alone. Both testosterone aromatization and HCG-induced intratesticular estrogen production contribute to total estrogen load. Blood work monitoring helps identify whether intervention is needed.
HCG with aromatase inhibitors
When estrogen rises too high on HCG protocols, aromatase inhibitors like anastrozole can help. These medications block the enzyme that converts testosterone to estradiol, reducing estrogen production.
However, aromatase inhibitors don't fully address HCG-induced estrogen for a specific reason. Much of the aromatization from HCG occurs within the testes themselves, where AI penetration is limited. Systemic AI doses that adequately suppress testicular aromatization often crash overall estrogen to problematic lows.
For men needing estrogen control on HCG, SERMs often work better than AIs.
Tamoxifen blocks estrogen receptors in breast tissue, preventing gynecomastia without reducing estrogen's beneficial effects on bone, brain, and cardiovascular health.
HCG with clomiphene or enclomiphene
Combining HCG with SERMs serves different purposes depending on the context. During PCT, HCG maintains testicular function while SERMs help restore pituitary LH production. The combination accelerates recovery compared to either alone.
For fertility purposes, this combination provides both direct testicular stimulation (HCG) and increased pituitary support (clomiphene). Some protocols use this approach when HCG alone hasn't restored adequate sperm parameters.
In ongoing therapy rather than recovery, using both simultaneously is less common. Men typically choose one or the other based on their specific goals and preferences.
HCG with FSH or HMG
For maximum spermatogenic stimulation, combining HCG with FSH provides both aspects of gonadotropin support. HCG stimulates Leydig cells for testosterone production while FSH supports Sertoli cells for sperm maturation.
HMG (human menopausal gonadotropin) contains both LH and FSH activity, providing combined stimulation in a single product. Research shows combined therapy achieves complete spermatogenesis in 86% of patients compared to 40% with HCG alone.
These combinations are typically reserved for men with significant fertility challenges, particularly those with hypogonadotropic hypogonadism affecting both LH and FSH. The added complexity and cost make them less suitable for general optimization purposes.
Legal status and obtaining HCG
The regulatory landscape around HCG has shifted in recent years, affecting availability and access. Understanding current status helps navigate options appropriately.
FDA-approved uses
In the United States, HCG is FDA-approved as a prescription medication for treating specific conditions including hypogonadism, male infertility, and cryptorchidism. Obtaining HCG requires a prescription from a licensed healthcare provider.
Recent regulatory changes have affected compounding pharmacies' ability to produce HCG. This has reduced availability through some channels and may have increased costs. The situation continues evolving, so checking current regulations matters when planning protocols.
Clinical access options
Men seeking HCG have several legitimate pathways.
Traditional endocrinologists and urologists prescribe HCG for appropriate medical indications. Men's health clinics and telehealth hormone optimization services often provide more accessible prescribing for TRT adjunct use.
For guidance on finding peptide therapy near you, our location guides cover options in major cities including Houston, Austin, Phoenix, Atlanta, Las Vegas, Scottsdale, and Miami.
Quality and sourcing considerations
Like any prescription medication, HCG quality varies by source. FDA-approved pharmaceutical products undergo rigorous testing and quality control. Products from other sources may lack these assurances.
When evaluating HCG sources, consider purity, potency verification, storage and handling during shipping, and reputation. Third-party testing provides independent verification of product quality when available.
For broader context on evaluating peptide solutions and sources, understanding quality markers helps make informed decisions.
SeekPeptides maintains resources helping members evaluate and verify product quality.
Monitoring and blood work for HCG users
Effective HCG use requires ongoing monitoring to optimize results and catch potential issues early. Blood work provides objective data that subjective symptom assessment cannot.
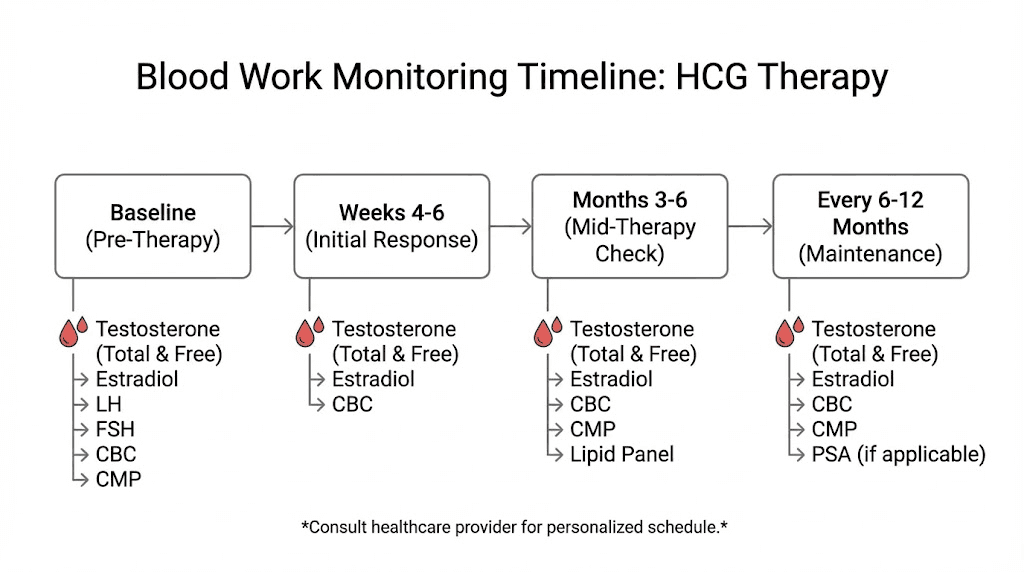
Essential tests to track
Total and free testosterone: These are your primary outcome measures. Effective HCG therapy should increase both values, though the magnitude depends on your specific protocol and individual response.
Estradiol (sensitive assay): Standard estradiol tests lack precision at male ranges. Request the sensitive or ultrasensitive assay for accurate readings. Rising estrogen on HCG is normal but requires attention if symptoms develop or levels climb excessively.
LH and FSH: These hormones provide insight into pituitary function. On HCG therapy, LH will typically suppress because your body senses adequate testicular stimulation. FSH may remain measurable unless fully suppressed by concurrent testosterone use.
Complete blood count: Testosterone-boosting therapies can increase red blood cell production. Monitoring hematocrit identifies if blood thickness becomes problematic, requiring intervention like blood donation or dose adjustment.
PSA (prostate-specific antigen): Baseline PSA before starting any testosterone-enhancing therapy establishes reference. Significant increases warrant urological evaluation, though modest rises often occur with testosterone elevation.
Testing schedule
Before starting HCG, obtain comprehensive baseline labs including all tests listed above plus general health markers like lipid panel and metabolic panel.
Recheck at six weeks after starting or changing doses. This timing allows sufficient period for hormone levels to stabilize while catching issues before they compound.
Once stable on a protocol, quarterly monitoring maintains oversight without excessive testing. More frequent checks may be warranted if adjusting doses or experiencing symptoms.
Semen analysis for fertility-focused protocols
Men using HCG for fertility should add semen analysis to their monitoring. Baseline analysis before treatment establishes starting point. Repeat analysis at three months and six months shows trajectory.
Key semen parameters include concentration (millions per milliliter), total count (concentration multiplied by volume), motility (percentage moving appropriately), and morphology (percentage with normal shape). Improvement in any or all of these suggests HCG is working. Lack of improvement after six months may indicate need for protocol adjustment or additional interventions.
Common questions and troubleshooting
Even with proper protocols, questions arise during HCG use. Understanding common issues and their solutions helps optimize outcomes.
HCG isn't raising my testosterone enough
If testosterone remains low despite HCG therapy, several factors might be at play. Insufficient dosing is the most common culprit. Men respond differently, and some need higher doses to achieve meaningful stimulation. Increasing dose incrementally, with monitoring, often resolves inadequate response.
Primary testicular failure limits HCG effectiveness. If the Leydig cells can't respond to stimulation, no amount of HCG will produce testosterone. Blood work showing high LH and FSH naturally (before HCG) suggests primary failure, which responds poorly to HCG.
Product quality issues occasionally explain poor response. If you've verified dosing is adequate and testicular function is intact, considering alternate sources may be worthwhile.
I'm experiencing estrogen-related side effects
Rising estrogen manifests as water retention, emotional sensitivity, decreased libido, or breast tissue changes. Blood work confirms whether estrogen is actually elevated or symptoms have other causes.
If estrogen is high, dose reduction often helps. Lowering HCG dose reduces testosterone production, which reduces aromatization substrate. This approach maintains therapy while limiting side effects.
Adding tamoxifen (10-20mg daily) blocks estrogen receptors in breast tissue without affecting estrogen elsewhere. This targeted approach prevents gynecomastia while preserving estrogen's benefits for bones, cardiovascular system, and cognition.
Aromatase inhibitors work but require careful dosing to avoid crashing estrogen. If using AI with HCG, start with low doses and monitor closely.
My testes aren't responding
Some men report continued testicular atrophy despite HCG therapy. This typically indicates insufficient dosing, product quality issues, or advanced atrophy requiring higher stimulation.
Try increasing dose to the higher end of recommended ranges, ensuring 500 IU minimum for each administration. Verify product storage and handling haven't compromised potency. Consider that recovery from significant atrophy takes time, months rather than weeks.
Should I cycle HCG or use it continuously?
For men on ongoing TRT, continuous HCG use maintains consistent testicular support. Cycling on and off allows atrophy during off periods, requiring recovery each time.
For PCT, HCG is inherently temporary, used during the transition to natural function restoration. In this context, discontinuing after the recovery period is appropriate.
For monotherapy, some practitioners recommend periodic breaks to assess baseline function. Others maintain continuous use. Individual circumstances and goals should guide this decision.
Frequently asked questions
Is HCG legal for men to use?
HCG is a legal prescription medication in the United States and most countries. It requires a doctor's prescription for medical uses including hypogonadism and fertility. Using HCG for legitimate medical purposes with proper prescription is legal, though regulations vary by location.
How quickly does HCG work for testosterone?
Most men notice testosterone increases within 2-4 weeks of starting HCG therapy. Blood work typically shows elevated levels by week 4-6. Symptom improvement follows testosterone elevation, with many men reporting benefits within the first month. For context on timelines, our guide on how long peptides take to work covers general expectations.
Can HCG be used without testosterone therapy?
Yes, HCG monotherapy is a viable option for men with mild hypogonadism who want to boost testosterone naturally while preserving fertility and testicular function. Studies show 40-80% testosterone increases with HCG alone. This approach works best for men with secondary hypogonadism where the testes function normally but lack adequate stimulation.
Does HCG cause testicular cancer?
No, HCG does not cause testicular cancer. In fact, HCG serves as a tumor marker for certain testicular cancers because some tumors produce HCG. If baseline HCG levels are elevated in men not using exogenous HCG, this warrants investigation. Administered HCG for testosterone support has no known association with cancer development.
Can I use HCG for weight loss?
The FDA explicitly states that HCG has not been proven effective for weight loss. Products marketed for this purpose lack scientific support. Any weight loss reported with "HCG diets" results from the extremely low-calorie restrictions, not the HCG itself. For metabolic support, explore fat burning peptides with actual evidence.
How do I store HCG after mixing?
Reconstituted HCG must be refrigerated at 36-46°F (2-8°C). It remains potent for 60-90 days when properly stored. Protect from light and avoid freezing. Before reconstitution, lyophilized HCG can be stored at room temperature though refrigeration extends shelf life. For more details, see our guide on how long reconstituted peptides last.
What happens if I stop taking HCG while on TRT?
Discontinuing HCG while continuing TRT leads to return of testicular atrophy over weeks to months as the testes lose stimulation. Fertility potential decreases as sperm production declines. Some men choose this when fertility is no longer a concern. Resuming HCG later can restore testicular function, though recovery takes time.
Is HCG the same as HGH?
No, HCG (human chorionic gonadotropin) and HGH (human growth hormone) are completely different hormones. HCG stimulates testosterone production in men. HGH affects growth, metabolism, and body composition. They serve different purposes and are not interchangeable. For information on growth hormone-related peptides, see our sermorelin and ipamorelin guides.
External resources
For researchers serious about optimizing their hormone protocols, SeekPeptides offers the most comprehensive resource available.
Evidence-based guides, proven protocols, and a community of thousands who've navigated these exact questions help members make informed decisions about HCG and other compounds in their optimization journey.